

Translate this page into:
Primary antiphospholipid syndrome presenting as thrombotic microangiopathy: Successful treatment with steroids, plasma exchange and anticoagulants
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Antiphospholipid syndrome (APS) often presents as a multisystem disorder characterized by recurrent arterial and venous thrombosis and pregnancy loss. We present a 46-year-old female who was admitted with oliguric acute renal failure. APS was suspected due to prolongation of activated partial thromboplastin time and history of miscarriages. Investigations for secondary causes were normal. Renal biopsy findings revealed thrombotic microangiopathy. A complete recovery of renal function was attained with a combination of plasma exchange and pulse methylprednisolone followed by oral steroids and warfarin. The case is presented for its rarity and therapeutic implications.
Keywords
Acute renal failure
anticardiolipin antibody
plasma exchange
primary antiphospholipid syndrome
thrombotic microangiopathy

Introduction
Antiphospholipid syndrome (APS) is characterized by the formation of antibodies to a variety of phospholipids and phospholipid-binding proteins. Renal manifestations vary from asymptomatic proteinuria to acute renal failure. The kidney appears to be a major target organ in both primary and secondary APS. An early detection of renal involvement will allow the initiation of anticoagulation to prevent recurrent thromboses and enable successful transplantation.[12]
Case Report
A 46-year-old female presented with 2 weeks history of generalized swelling and oliguria. There was no history of hematuria, antecedent throat, or skin infection. Medication history was not significant. Obstetric history included two second-trimester spontaneous abortions and two live births. Both the live births were home deliveries at term without any antepartal or postpartal complications. There was no history of hypertension or hyperglycemia during or after pregnancies.
Physical examination revealed pallor, anasarca, pulse rate 92/min, blood pressure of 150/100 mmHg, temperature 36.9°C, and respiratory rate 15/min. There was no skin rash, arthritis, Raynaud's phenomenon, or oral ulcers. The 24-h urine output was 200 ml. Investigations included hemoglobin 11.1 g/dl, total leucocyte count 7.4 × 1000/ mm3, platelet count 90,000 cells/mm3, reticulocyte count 1.2%, serum creatinine 3.7 mg/dl , uric acid 7 mg/dl, calcium 9.6 mg/dl, inorganic phosphorus 3.6 mg/dl, bilirubin 0.6 mg/dl , total protein 5.8 g/dl, albumin 3.6 g/dl, AST 12 IU/l, ALT 14 IU/l, alkaline phosphatase 24 U/l, antistreptolysin-O titer <200 units, LDH 120 IU/l, and C-reactive protein 0.5 mg/dl. Peripheral smear was normocytic, normochromic and there was no evidence of hemolysis. Direct and indirect Coombs tests were negative. HBsAg and anti-HCV antibody ELISA were negative. Chest X-ray was normal, and urine and blood cultures were sterile. Ultrasound revealed normal-sized kidneys with normal corticomedullary differentiation. Doppler ultrasound of renal vessels was normal. Antinuclear antibody (negative), anti-dsDNA, and ANCA titers were within normal limits. Complement levels (C3 and C4) were normal. Urine analysis showed 3+ proteinuria, 1–2 white blood cells per high-power field, 15–20 RBC per high-power field, and no casts. The patient had prolonged APTT of 54.5 s (control 29 s) and prothombin time of 18.5 s (control 12.1 s). The anticardiolipin antibody IgG titer was 4.2 GPL and the IgM titer was 183 MPL units. The lupus anticoagulant test was negative. The hypercoagulability panel (fibrinogen, protein S, protein C, antithrombin III) was within normal limits. With a history of recurrent fetal loss and elevated ACL titers, the diagnosis of APS was considered. As plasma infusions did not achieve correction of APTT, patient was started on plasma exchange with fresh frozen plasma. The patient required alternate day hemodialysis of 4-h duration for the maintenance of volume status. APTT was normalized and the platelet count improved to 156 × 1000 cells/ mm3 after four sessions of alternate day plasma exchange (40 ml/kg). An ultrasound-guided percutaneous renal biopsy was done. Light microscopy showed glomeruli showing intracapillary fibrin thrombi with segmental fibrinoid necrosis and mesangiolysis [Figure 1]. The tubules showed focal atropy and distalization due to focal acute tubular necrosis. The interstitium showed minimal lymphomononuclear infiltrate. The blood vessels were normal. Immunofluorescent micrography revealed fibrin deposition with the absence of specific immunoglobulin or complement (C3, C1q) deposits. With prolonged APTT and thrombotic microangiopathy on renal biopsy, we considered the diagnosis of primary antiphospholipid syndrome (PAPS). A detailed evaluation of clinical and laboratory data excluded secondary APS. Anticoagulation was initiated 48 h postbiopsy with heparin, continued for 5 days, and later overlapped with oral warfarin. The patient was given pulse methylprednisolone (15 mg/ kg, three doses) and continued on oral prednisolone 1 mg/ kg. Plasma exchange was continued for a total of eight sessions. After 2 weeks of therapy with oral steroids and warfarin, renal function returned to normal. Oral steroids and warfarin were continued up to 12 weeks. The anticardiolipin antibody IgM titer was 142 MPL units at 6 weeks and 86 MPL units at 12 weeks. The oral steroid was tapered after 12 weeks and oral warfarin was continued (target INR 2). At 24 weeks, the patient had normal renal function with subnephrotic protenuria of 800 mg/day. ANA and anti-dsDNA were negative at the end of 24 weeks. At 12-month follow-up, the patient had normal renal functions, 24-h urine protein 150 mg per day, and a anticardiolipin antibody titer of 122 MPL units (IgM). The patient is presently on oral anticoagulation with warfarin with a maintenance INR of 2.
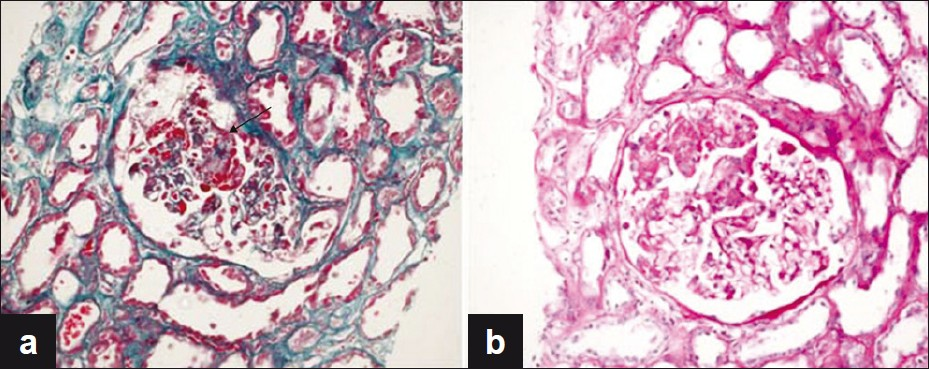
- Glomerulus showing segmental fibrinoid necrosis (arrow) and mesangiolysis, with dilatation of glomerular capillary loops. (a) Masson's trichrome stain; (b) periodic acid Schiff stain; magnification, ×200
Discussion
First described by Hughes in 1983,[3] antiphospholipid antibodies associated with vaso-occlusive events without any underlying disease process is termed as the PAPS. Most common manifestations include deep vein thromboses, pulmonary emboli, strokes, and myocardial infarction. The patient described herein presented with acute renal failure and reinstates the fact that nephropathy may be the only presentation of PAPS in the absence of other thrombotic processes.[45]
Renal abnormalities are present in approximately 9% of patients with PAPS,[6] and are also seen in secondary APS.[7] Hypertension is the most common manifestation (93%) followed by reduced GFR (87%), proteinuria (75%), and hematuria (56%).[89] Renal failure can be acute or insidious with a progressive decline in renal function and hypertension.[10]
Thrombosis can manifest as renal artery thrombosis or stenosis, thrombotic microangiopathy, renal vein thrombosis, and cortical infarcts. Renal histology in primary APS shows arteriosclerosis (75%), fibrous intimal hyperplasia (75%), focal cortical atropy (62%), or thrombotic microangiopathy (31%).[8] Glomerular changes such as mesangial IgA deposits, membranous nephropathy, and proliferative glomerulonephritis have also been described.[6]
Thrombotic microangiopathy (TMA) is a noninflammatory thrombotic vasculopathy commonly involving the glomerular capillaries, preglomerular arterioles, and small interlobular arteries. Though TMA can occur under various other conditions,[11] the presence of TMA in the setting of suspected APS is considered characteristic of APS nephropathy.[12] Histologically, renal biopsy shows focal or diffuse microangiopathic changes with fresh and old recanalized thrombi. The glomerular capillaries are occluded by fibrin thrombi and proliferating endothelial cells bulging into the vascular lumen. Vascular occlusion is totally noninflammatory and immunoflorescence is positive only for fibrin. Electron microscopy can show wrinkled segments of the basement membrane with straighter, thin basement membrane sections adjacent to the endothelium. Our patient's biopsy findings were consistent with thrombotic microangiopathy and there was no evidence of vasculitis.
Therapy for PAPS has not been standardized. In a literature review of 46 patients,[13] steroids were the most common treatment (69%), followed by plasma exchange (PE) (62%), anticoagulant or antithrombotic agents (48%), immunosuppressive agents (29%), and immunoglobulins (12%). Since the disease is characterized by recurrent thrombotic events, the early initiation of anticoagulants remains the key to achieve remission.[14] Regarding the intensity of anticoagulation, randomized controlled trials with two intensities of warfarin concluded that both moderate (INR 2–3) and high intensity anticoagulation (INR 3–4) are similarly protective in APS patients after the first thrombosis. Once patients are established on warfarin, aspirin does not offer any added advantage.[12] Methylprednisolone, anticoagulants, cyclophosphamide, and plasma exchange have been used in various combinations to achieve renal recovery.[15–17]
This case report provides further evidence to support the combination of steroid, warfarin, and plasma exchange to achieve a complete recovery of renal function in APS nephropathy. The anticardiolipin antibody titers also decreased following treatment suggesting a probable direct pathogenetic role of antiphospholipid antibodies.
Conclusions
Acute renal failure is a rare presentation of primary APS. PAPS must be considered in the differential diagnosis of acute renal failure in patients with thrombotic microangiopathy or prolonged APTT. Immunosupression and plasma exchange bring about significant improvement in prognosis. Further research is required to establish the pathogenesis of primary APS and derive uniform treatment stratergies. Meanwhile, we suggest early aggressive combination therapy which is essential to obtain a favorable response in primary APS.
Source of Support: Nil
Conflict of Interest: None declared.
References
- End-stage renal disease from glomerulonephritis associated with anti-phospholipid syndrome. Pediatr Nephrol. 2004;19:812-4.
- [Google Scholar]
- Thrombosis, abortion, cerebral disease, and the lupus anticoagulant. Br Med J (Clin Res Ed). 1983;287:1088-9.
- [Google Scholar]
- Is it possible to diagnose primary anti-phospholipid syndrome (PAPS) on the basis of renal thrombotic microangiopathy (PAPS nephropathy) in the absence of other thrombotic process? Ren Fail. 2003;25:1043-9.
- [Google Scholar]
- Reversible renal failure in the primary antiphospholipid syndrome--a report of two cases. J Am Soc Nephrol. 1993;4:28-35.
- [Google Scholar]
- Renal involvement in primary antiphospholipid syndrome: Retrospective analysis of 160 patients. Clin J Am Soc Nephrol. 2010;5:1211-7.
- [Google Scholar]
- The Intrarenal vascular lesions associated with primary antiphospholipid syndrome. J Am Soc Nephrol. 1999;10:507-18.
- [Google Scholar]
- Antiphospholipid syndrome (APS) nephropathy in catastrophic, primary, and systemic lupus erythematosus-related APS. J Rheumatol. 2008;35:1983-8.
- [Google Scholar]
- Endstage renal failure in primary antiphospholipid syndrome-case report and review of literature. Rheumatology (Oxford). 2003;42:1128-9.
- [Google Scholar]
- Antiphospholipid syndrome nephropathy in patients with systemic lupus erythematosus and antiphospholipid antibodies: Prevalence, clinical associations, and long-term outcome. Arthritis Rheum. 2004;50:2569-79.
- [Google Scholar]
- Renal manifestations of the antiphospholipid syndrome. Curr Rheumatol Rep. 2009;11:52-60.
- [Google Scholar]
- Thrombotic microangiopathic haemolytic anaemia and antiphospholipid antibodies. Ann Rheum Dis. 2004;63:730-6.
- [Google Scholar]
- Antiphospholipid antibody syndrome and renal disease. Curr Opin Nephrol Hypertens. 2001;10:175-81.
- [Google Scholar]
- A case of primary antiphospholipid antibody syndrome with acute renal failure showing thrombotic microangiopathy. Am J Nephrol. 1999;19:594-8.
- [Google Scholar]
- Renal involvement in primary antiphospholipid syndrome and its response to immunosuppressive therapy. Lupus. 2003;12:760-5.
- [Google Scholar]
- A case of primary antiphospholipid antibody syndrome with severe nephrotic syndrome showing remarkable endothelial cell damage in the capillary lumen. Nippon Jinzo Gakkai Shi. 1997;39:431-7.
- [Google Scholar]




