

Translate this page into:
Emphysematous pyelonephritis: Outcome with conservative management
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Emphysematous pyelonephritis is a life-threatening condition characterized by necrotising gas forming infection of the renal parenchyma. We describe eight patients seen over a period of 2 years, 62.5% males and 37.5% females with age range between 21 and 65 years. About 75% patients had diabetes mellitus. Six patients were managed conservatively. One patient required nephrectomy with percutaneous drainage and one patient died without surgical intervention.
Keywords
Diabetes mellitus
emphysematous pyelonephritis
urinary tract infection

Introduction
Emphysematous pyelonephritis (EPN) is an acute necrotising gas producing infection of the renal parenchyma with grave prognosis if not treated in time.[1] Predominantly caused by bacterial pathogens, fungal etiology has been implicated in many case reports.[23] EPN is still an uncommon disease with no clear-cut guidelines for diagnosis and management. We therefore, report our experience on the course and outcome of the disease with conservative versus surgical management.
Materials and Methods
A total of eight patients with EPN (5 males and 3 females), with age range between 21 years and 65 years were admitted in our hospital during the 2-year period. Patients were classified into four classes using the classification system proposed by Huang and Tseng.[1] Risk factors for EPN in the form of diabetes, chronic kidney disease, immunosuppression, and obstruction were noted. Diagnostic work-up and therapy was at the discretion of attending doctor. The outcome was reported as improvement or death.
Results
All the patients presented to Emergency Department. Two patients were managed in the Intensive Care Unit (ICU) and rest were managed in the wards. On the total, 62.5% were males and 37.5% were females of which 75% patients had diabetes mellitus. One patient did not have any risk factor. Four patients had the presence of two or more than two adverse prognostic factors. Other features are shown in Table 1.
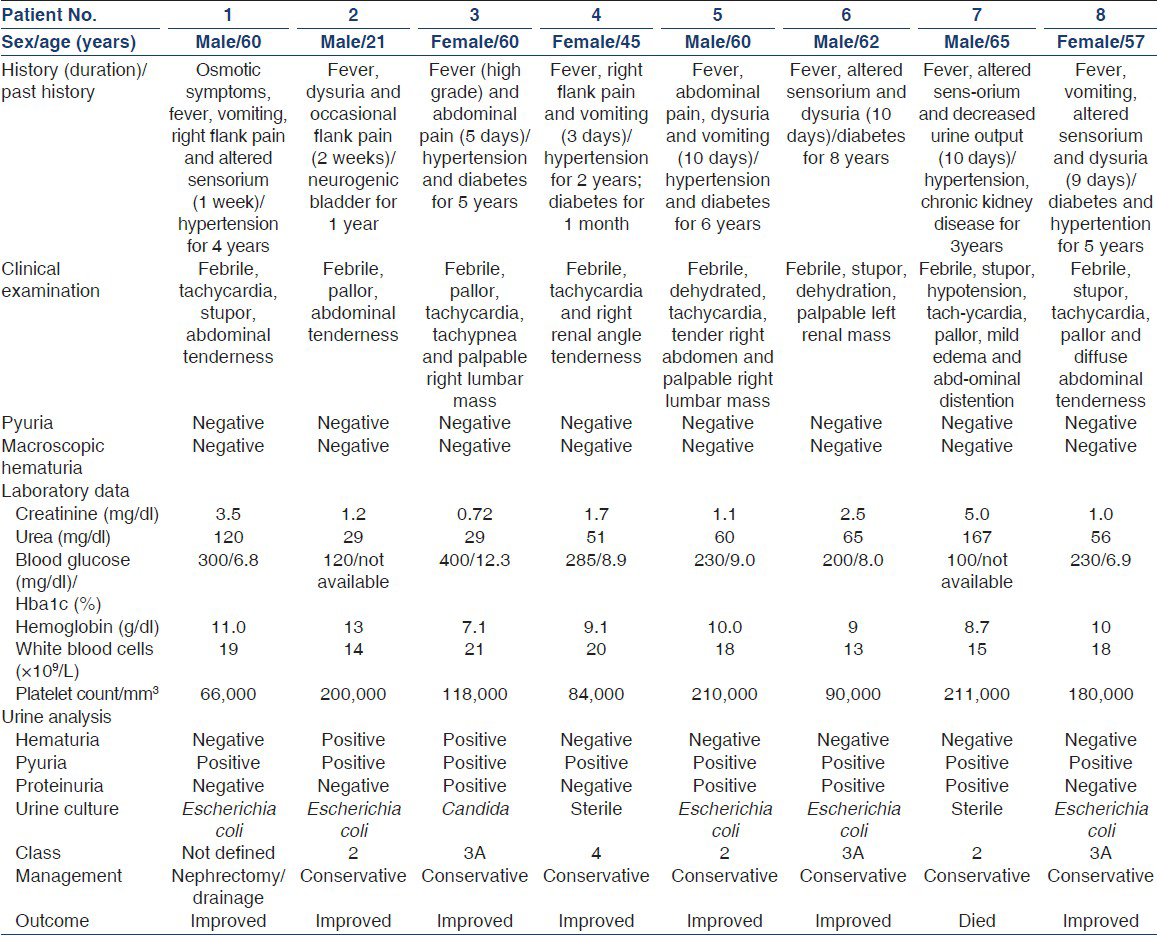
Six patients were managed conservatively. Three patients had class 3A disease, two patients had class 2 and one patient had class 4 disease. Two patients had ≥2 bad risk factors. All patients improved with conservative management. One patient who presented with an unusual class had the presence of 3 risk factors and was managed with nephrectomy and improved. One patient with class 2 disease and the presence of >2 risk factors showed rapid deterioration and died within 24 h of admission.
The clinical presentation of the patients is shown in Table 1. Fever was present in all patients. 62.5% patients had abdominal orflank pain and 50% patients had vomiting at presentation. 50% patients had altered sensorium and 75% patient had hypertension and diabetes. All patients were febrile. 75% patients had abdominal tenderness and 37.5% patient had palpable abdominal mass.
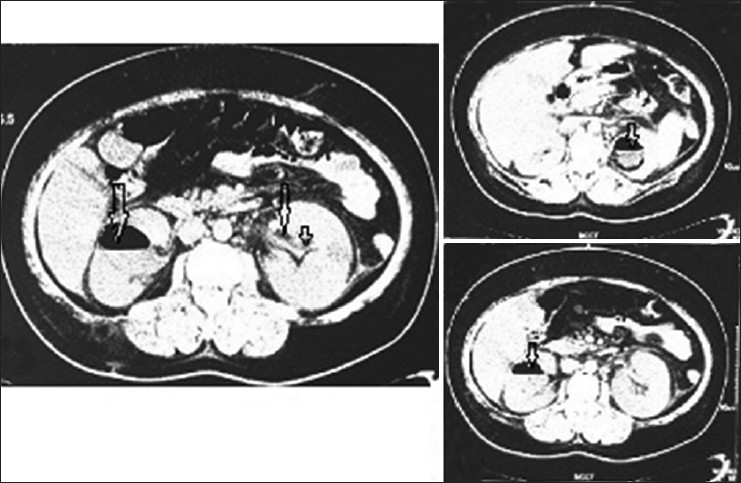
Two patients had unusual presentation and progression. Case no. 1 was an elderly male who was first time detected diabetes mellitus at presentation of the disease with no prior history suggestive of diabetes mellitus. CT imaging of the abdomen showed gas in the right renal fossa with streaks of kidney tissue discernable. Gas was present in the perinephric space, perihepatic area, and subcutaneous tissue [Figure 1]. Right nephrectomy with pus drainage was carried out. Patient was managed in ICU and showed full clinical recovery.

- Undefined class of emphysematous pyelonephritis. (a) Non-contrast cross-sectional computed tomography (CT) picture of the abdomen showing gas in right renal fossa (white arrow), strands of renal tissue (green arrow) and gas in subcutaneous tissue (red arrow). (b) CT picture of the abdomen showing similar findings in coronal section. (c) Nephrectomy specimen of the same patient showing necrosis (white arrows) and areas of papillary necrosis (red arrows). (d) Post-surgery CT picture showing resolution of earlier findings with catheter in place (white arrow)
Case no. 2 was a young male with no obvious significant past history presented with features of pyelonephritis. Patient was on indwelling catheter for past 1 year for neurogenic bladder (secondary to trauma). Patient did not have any known risk factors of EPN. Imaging studies showed emphysematous changes in the right kidney with fractured Foleys catheter tip inside the bladder [Figure 2a]. Patient was managed with antibiotics and catheter tip was removed by cystoscopy. Patient was discharged after 5 days of stay.

- Class 2 emphysematous pyelonephritis. Right, X-ray showing Foley's catheter tip within the urinary bladder (black arrows). Left, computed tomography abdomen showing EPN in the right kidney (black arrow)
Case no. 3 was a diabetic female who presented with high grade fever and abdominal pain. Patient was febrile, tachypneic, and had palpable abdominal mass. Patient had class 3A disease [Figure 2b] and Candida was grown from urine. Case no. 4 was an adult diabetic female who presented with fever, abdominal pain, and vomiting. She was febrile and had tender abdomen. She had class 4 EPN [Figure 3] and two bad prognostic factors in the form of renal failure and thrombocytopenia. The clinical characteristics of other patients are shown in Table 1.
- Class 4 emphysematous pyelonephritis. Computed tomographic scan abdomen showing emphysematous changes in both the kidneys (black arrows)
All patients were started on intensive antibiotic regimen and modification carried out as per culture sensitivity. Seven patients were managed with two antibiotics and one was treated with antifungals. One patient required cystoscopy and removal of foreign body in the form of fractured catheter tip. Six patients showed full improvement on conservative management. One patient presented with undefined class of disease and had the presence of three risk factors. Patient did not improve with conservative management and required nephrectomy. One patient died even on intensive antibiotic regimen. The average duration of admission in all patients was 8-14 days.
Discussion
EPN is an uncommon life-threatening condition characterized by the production of gas within the renal parenchyma and perirenal space.[45] The common predisposing factors include Diabetes mellitus, urinary tract obstruction, polycystic kidneys, end stage renal disease and immunosuppression.[1] Escherichia coli is the most common pathological agent incriminated in 69% to 90% of the cases.[6]
EPN being more common in females than males has been found in many studies.[17] Nearly, 62.5% patients in our series were males. Also, 75% patients had diabetes mellitus and one patient had chronic kidney disease. One patient did not have any of the known risk factors of EPN. He was on indwelling catheter for last 1 year and presented with fractured Foleys tip within the urinary bladder. tThe exact mechanism of EPN in this patient in not obvious. However, the migration of catheter tip into the left ureter and retrograde infection could only be speculated although no features of obstruction were apparent. Non-resolving upper urinary tract infection leading to EPN without underlying risk factors is not reported to our best knowledge.
One patient showed extensive disease in the form of gas in the renal fossa, perinephric area, and subcutaneous tissue with only minimal renal tissue discernable on CT abdomen. This patient could not be classified in the classification system proposed by Huang and Tseng. This was the only patient managed with nephrectomy and improved fully.
Risk factors having prognostic implication include altered sensorium, thrombocytopenia, hypotension, and acute renal failure.[1] Factors such as age, sex, site of infection, and blood glucose level have not been found to have value in defining prognosis.[8] Huang and Tseng found that patients with class 1 and 2 disease have excellent prognosis with percutaneous drainage (PCD) combined with antibiotics. Patients with class 3 and 4 disease with <2 risk factors can be tackled with PCD combined with antibiotics. In patients with extensive disease and ≥2 risk factors, nephrectomy should be the best and immediate option.[1] In our series, two patients with class 4 and 3A disease had ≥2 risk factors and were managed with antibiotics only without surgery. One patient with underlying chronic kidney disease and class 2 EPN had more than two risk factors and died within 24 h of admission. It is therefore, clear that the mortality in patient of EPN of any class is largely determined by the presence of risk factors.
Conclusion
Conservative management should be an initial approach in those patients with less than two risk factors irrespective of the class of the disease. Surgery should not be delayed in any case when indicated. The sample size in our study was small and this fact needs consideration while interpreting the results.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Emphysematous pyelonephritis: Clinic radiological classification, management, prognosis, and pathogenesis. Arch Intern Med. 2000;160:797-805.
- [Google Scholar]
- Emphysematous Pyelonephritis Caused by Candida Parapsilosis: An Unknown Etiological Agent. North Am J Med Sci. 2012;4:364-6.
- [Google Scholar]
- Bilateral emphysematous pyelonephritis caused by Candida glabrata: An exceptional entity. Nephrol Ther. 2010;6:541-3.
- [Google Scholar]
- Acute gas-producing bacterial renal infection: Correlation between imaging findings and clinical outcome. Radiology. 1996;198:433-8.
- [Google Scholar]
- Urinary tract infections in patients with diabetes mellitus. In: Rose BD, ed. UpToDate. Vol 15. 2007. CD-ROM
- [Google Scholar]




