

Translate this page into:
Giant migratory enterolith mimicking vesical calculus
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 55-year-old female presented with complaints of burning micturition, left flank pain, and occasional discomfort in suprapubic region for last 6 years. She was diagnosed to have left nephrolithiasis and vesical calculus and managed conservatively whenever her symptoms aggravated. Plain abdominal radiograph revealed a radio-opaque shadow in left renal fossa. Lamellated radio-opacity with central lucency was also seen in the midline in pelvis [Figure 1]. At first instance, we thought we were dealing with left renal and vesical calculi. Intravenous urography confirmed left nephrolithiasis. However, the radio-opacity in pelvis was outside the urinary bladder [Figure 2]. In addition, the opacity migrated toward the right hemipelvis. Contrast-enhanced computed tomography of the abdomen revealed the opacity to be a giant enterolith measuring 4 × 2.7 cm in the ileal loop [Figure 3], which migrated toward the left hemipelvis. No proximal bowel dilatation/stricture was noted. Patient refused to undergo any surgical procedure and is on regular follow-up.
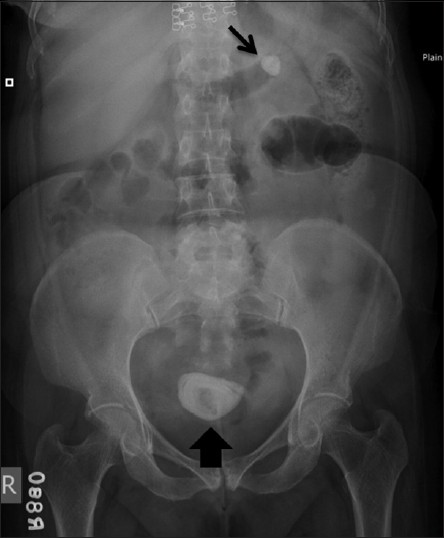
- Radiograph of kidneys-ureters-bladder showing radio-opaque shadow in left renal fossa (arrow) at level of transverse process of L1 vertebra and a lamellated oval radio-opacity in pelvis (arrowhead)

- Intravenous urography confirming left nephrolithiasis in the upper pole calyx with caliectasis (arrow). The radio - opacity in the pelvis is seen to lie outside the urinary bladder (arrowhead). Normal excretion is seen on the right side

- Axial computed tomography abdomen showing hyperdense giant enterolith (black arrow) in ileal bowel loop separate from the urinary bladder (white arrow)
Enteroliths, first described in 1915, are commonly found in horses. In humans, enteroliths are of three types - containing bile acids, calcium oxalate, or phosphate.[1] The maximum size reported is more than 6 cm, and 1400 in number were found in a patient of carcinoma colon.[2]
Enteroliths are formed due to intestinal stasis as in diverticulae, or congenital/acquired strictures (intestinal tuberculosis, Crohn's disease, carcinoid tumor, posttraumatic or postsurgical strictures, radiation enteritis, etc.).[3] High calcium content in the diet is also a predisposing factor; stasis results in alteration of bacterial flora, leading to bacterial overgrowth; conversion of soluble cholic acid into insoluble deoxycholic acid. Glycine and taurine bile salts are cleaved to precipitate such unconjugated bile acids in the intestinal lumen, thus forming the enterolith. Stasis may also result in enzymatic hydrolysis of the biliary lecithin, conditioning the appearance of free fatty acids that quickly combine with calcium ions to form insoluble "calcium soaps".[4] The chemical composition of enteroliths depends on where they are formed and the pH of the intestinal lumen. The relatively high acidity of the proximal duodenum and jejunum allows precipitation of bile acids, particularly cholic acid, which are radiolucent. The alkaline lower part of the small intestine is conducive to the precipitation of calcium and hence enteroliths in this location are radio-opaque.
Patients may present with features of recurrent intestinal obstruction, ulceration, malaena, perforation. Radiologically, enteroliths are seen as migrating lamellated radio-opaque shadow with central lucency. Differential diagnoses of such calcified pelvic opacities include enteroliths, appendicolith, calculus, teratoma, calcified lymph nodes, multiple gallstones (gallstone ileus), foreign bodies, calcified fibroid, etc., Recommended treatment is the removal of the stone by enterotomy, and resection of the abnormal intestinal loop.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Enterolithiasis complicating eosinophilic enteritis: A case report and review of literature. World J Gastrointest Surg. 2009;1:68-70.
- [Google Scholar]
- Small-intestinal enteroliths - Unusual cause of small-intestinal obstruction: Report of three cases. Dis Colon Rectum. 1999;42:676-9.
- [Google Scholar]




