

Translate this page into:
Takayasu arteritis: Association with mesangioproliferative glomerulonephritis in a 9-year-old child
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
A 9-year-old boy presented with anasarca, cola-colored urine and oliguria for 1-week. There was no history of rash, pyodermas, pharyngitis, jaundice or arthritis. Nine months ago, he was diagnosed to have Takayasu arteritis (TA) elsewhere based on hypertension (blood pressure 132/90 mm Hg) and absent left radial and dorsalis pedis pulses, along with angiographic involvement of thoracic and abdominal aorta. He had elevated erythrocyte sedimentation rate (40 mm/h) at that time. He subsequently underwent stenting of thoracic and abdominal aorta. He was treated with prednisolone, aspirin, clopidrogel and carvedilol, and became asymptomatic. There was no edema, hematuria or proteinuria at that time.
At entry, he was conscious. Blood pressure was 160/110 mm Hg, and all peripheral pulses were palpable. Ophthalmological evaluation was normal. Systemic examination revealed anasarca and features of congestive heart failure. There was no abdominal bruit, pulse deficit, or blood pressure discrepancy in the limbs. Urinalysis showed red blood cell casts and 3 + albuminuria. Serum creatinine was 0.6 mg/dl, serum cholesterol 150 mg/dl, and serum albumin 2.4 mg/dl. Antistreptolysin-O, antideoxyribonuclease B and C3 levels were normal. Antinuclear antibody, hepatitis B surface antigen and HIV serology were negative. Chest X-ray showed cardiomegaly and thoracic aorta stent. Renal ultrasonogram was normal. Echocardiography showed dilated cardiomyopathy with global hypofunction (ejection fraction 30%).
He required sodium nitroprusside infusion for blood pressure control followed by amlodipine. Renal biopsy showed mesangioproliferative glomerulonephritis [Figure 1]. He was treated with prednisolone, furosemide and enalapril. Prednisolone (2 mg/kg body weight) was administered daily for 4 weeks followed by tapering over the next 4 weeks. After 2 months, he became free of proteinuria and hypertension. Microscopic hematuria continues to persist.
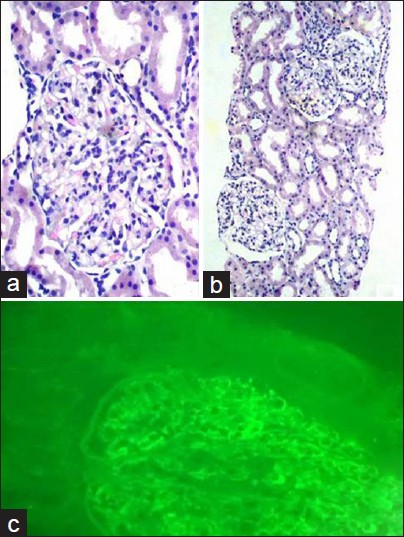
- (a) Section shows a single enlarged glomerulus with diffuse mesangial proliferation (H and E stain, ×400) (b) Section shows glomeruli with diffuse mesangial proliferation. Tubular and interstitial compartment are within normal limits (H and E stain, ×100) (c) Section shows granular deposits of IgM in mesangium and glomerular capillary wall (fluorescein isothiocyanate stain, ×400)
Takayasu arteritis is a common large vessel arteritis in children. Our patient had angiographic abnormality showing narrowing of the aorta, absent peripheral pulses and hypertension, thereby fulfilling the European League Against Rheumatism/Pediatric Rheumatology European Society criteria for TA.[1] The most common renal manifestations of TA are renovascular hypertension and ischemic glomerulopathy.[2] The latter is characterized by decrease in renal size, and tubulointerstitial atrophy.[3] These features were absent in our patient. Primary glomerulonephritis is uncommon in TA. Anecdotal reports of primary glomerulonephritis exist, pertaining mostly to adults and include membranoproliferative glomerulonephritis, membranous glomerulonephritis, IgA nephropathy, focal segmental glomerulosclerosis, and mesangioproliferative glomerulonephritis.[4]
Mesangioproliferative glomerulonephritis has been poorly documented in children;[5] and not from India. Our observations, along with other reports, support the view that TA may induce glomerular disease as part of its histopathological expression, or point toward a common immunological mechanism for glomerular or vasculitic involvements in these patients.[45]
References
- EULAR/PReS endorsed consensus criteria for the classification of childhood vasculitides. Ann Rheum Dis. 2006;65:936-41.
- [Google Scholar]
- Ischaemic nephropathy secondary to atherosclerotic renal artery stenosis: Clinical and histopathological correlates. Nephrol Dial Transplant. 2010;25:3615-22.
- [Google Scholar]
- Mesangioproliferative glomerulonephritis, antiphospholipid antibodies, and Takayasu's arteritis - is there a link? Nephrol Dial Transplant. 1998;13:991-3.
- [Google Scholar]
- Takayasu's arteritis associated with glomerulonephritis. A case report. Am J Dis Child. 1978;132:1009-13.
- [Google Scholar]




