

Translate this page into:
Carotid intima-media thickness as a marker of atherosclerosis in hemodialysis patients
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Atherosclerotic changes in carotid arteries of hemodialysis (HD) patients reflect global atherosclerotic changes in vasculature. Carotid intima-media thickness (CIMT) can be used for atherosclerosis prediction and assessment of cardiovascular risks in HD patients, and thus screening high-risk patients. In this cross-sectional study, CIMT was measured using ultrasonography (B-mode with 5-10-MHz multifrequency linear probe) in HD patients in our hospitals. Additionally, we assessed the relationship between their CIMT and some cardiovascular risk factors. A total of 62 HD patients (64.5% male) were included. Age, body mass index, low-density lipoprotein, fasting blood sugar, history of diabetes mellitus and cardiovascular disease, serum albumin, and duration and adequacy of HD in study patients had significant association with their CIMT. There were no significant relationships between CIMT and patient's gender, smoking, serum calcium, phosphate, calcium x phosphate product, hemoglobin, and uric acid level. More diagnostic modalities must be performed for detecting the impact of atherosclerosis on HD patients with high CIMT.
Keywords
Atherosclerosis
cardiovascular disease
carotid artery
intima-media thickness
hemodialysis

Introduction
Cardiovascular disease, mortality, and morbidity are more frequent in hemodialysis (HD) patients than in the general population, even in HD patients aged less than 45 years.[1] In European countries, cardiovascular disease (CVD) is the cause of death in 51% of HD patients and 37% of renal transplant patients.[2] More than 55% of mortality in HD patients in New Zealand and Australia is related to CVDs.[1]
Myocardial infarction and stroke in general population are associated with increase in intima-media thickness (IMT) of carotid arteries.[34] Chronic kidney diseases, especially in the end stage, is known as an independent predictor of carotid arterial IMT.[5] Some studies revealed that the prevalence of IMT in carotid artery of HD patients is higher than that in age- and gender-matched general population.[6]
Noninvasive tests are necessary for the diagnosis of CVDs, especially atherosclerotic changes in HD patients. There are some hypotheses that IMT in carotid artery might be one of the long-term predictors of survival outcomes in HD patients. B-mode ultrasound imaging is one of the tools used for the diagnosis of atherosclerotic changes.[37] This study was designed for determining the IMT of carotid artery in HD patients of Imam Khomeini Hospital between March and December 2007.
Materials and Methods
A total of 62 HD patients of Imam Khomeini hospital (Tehran, Iran) were included in this cross-sectional study between March and December 2007. Ethical clearance for the study was obtained from the Ethical Committee of Tehran University of Medical Sciences, and study methods were described clearly to patients and informed consent was obtained. Patients with acute kidney injuries and those with interventions on their carotid artery such as surgery or stent insertion were excluded.
History of cigarette smoking, HD duration, past history of CVD in patients and their first relatives, history of diabetes mellitus, and causes of renal failure were recorded. Urea reduction rate (URR) was calculated by dividing the difference between pre- and post-dialysis blood urea nitrogen (BUN) by pre-dialysis BUN. Arterial blood pressure was measured before HD session and body mass index (BMI) was calculated after that.
After 12-h fasting and in the beginning of HD session, serum level of calcium, phosphorus, uric acid, hemoglobin, albumin, creatinine, and lipid profile (triglyceride, total cholesterol, high-density lipoprotein, and low-density lipoprotein [LDL] were checked. To avoid probable bias, the radiologist was blinded ot the patient history and diagnosis.
Carotid intima-media thickness (CIMT) was measured at a distance of 1 cm from the carotid bulb with B-mode ultrasonography (multifrequency 5-10-MHz linear probe; Siemens, Sonoline G, Germany) by a single expert radiologist. The patients were made to lie in supine and extended neck position and ultrasonography was performed on three points on carotid arteries (common carotid, bifurcation point, and proximal of internal carotid arteries). Three images with the highest clarity through cine loop were selected and the mean of maximum CIMT was measured in each carotid artery of the HD patients. Ultrasound examination was repeated at the next visit during next month in five randomly selected patients for assessment of intra-observer reproducibility.
Statistical analysis
Data were analyzed using SPSS for Windows version 16. Quantitative variables were presented by central indices (mean and standard error of mean) and qualitative variables were presented by frequency tables (frequency and percentages). Mean of IMT between qualitative groups was compared with independent sample t-tests. Correlation analysis was used for the assessment of relationship between quantitative variables. Multiple logistic regression models were used for ruling out confounding variables. A two-tailed significance level of 0.05 was used to detect difference between variables.
Results
This study was performed on 62 (40 males) HD patients for assessment of atherosclerotic changes. Age and HD duration were 52.8 ± 14.6 years and 69 ± 58 months, respectively. Among the study patients, 32 (51.6%) patients had a history of CVDs in their families and 13 (21%) patients smoked. On all, 53 (58.8%) and 22 (35.5%) patients had a history of hypertension and diabetes, respectively. Diabetic nephropathy and hypertension were the most frequent causes of renal failure in our patients.
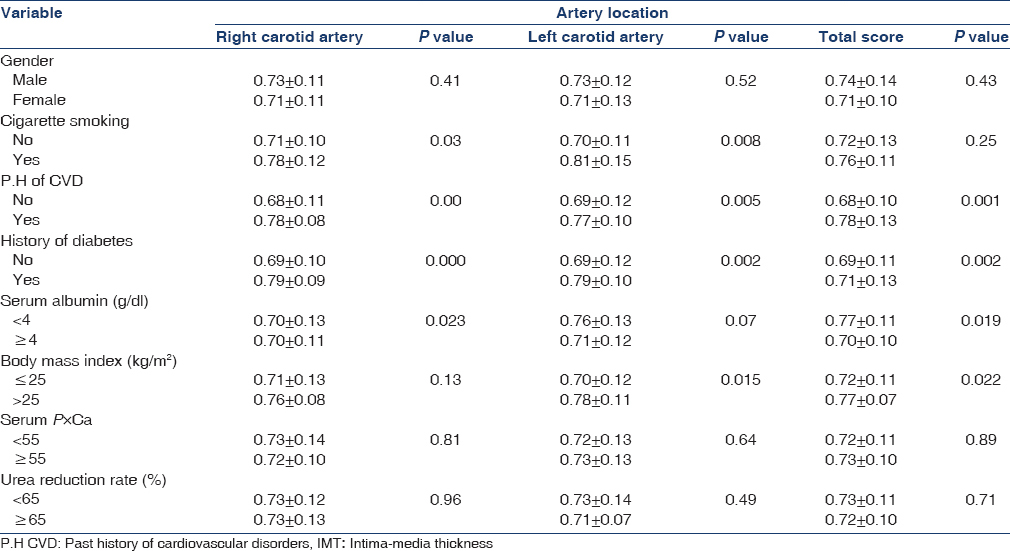
According to the ultrasonography results, the highest CIMT was found in the bifurcation point in the right (0.78 ± 0.18 mm) and left (0.77 ± 0.16 mm) carotid arteries, and internal carotid artery in the right (0.64 ± 0.14 mm) and left (0.66 ± 0.15 mm) sides had lowest CIMT. Patients’ characteristics and serum values are presented in Table 1.
Correlation analysis of CIMT with quantitative study variables in our study revealed a significant correlation between CIMT and FBS, LDL, URR, diastolic blood pressure, BMI, and HD duration. Details of other correlations are presented in Table 2.

We considered CIMT more than 0.75 mm as carotid atherosclerosis. The mean of quantitative variables was compared in patients with and without remarkable carotid atherosclerosis. Details of these comparisons are presented in Table 3.

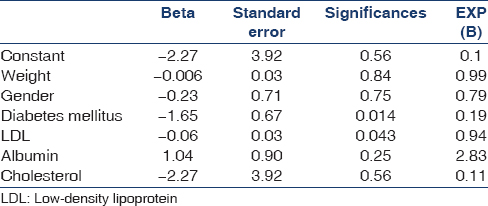
In logistic regression analysis, only diabetes and LDL were included in the model and were known as independent predictors of CVD in HD patients [Table 4].
Discussion
Carotid arteries are mirrors of coronary arteries, and atherosclerotic changes in each of them are related to the other site. Atherosclerotic changes in carotid arteries can cause morbidity and mortality by thrombosis in patients with coronary artery diseases.[8] Mean of CIMT in cigarette smoking patients was significantly higher than that in nonsmoking patients. Similar to our study, Dzitovea et al.'s[9] study reported that patients with a history of cigarette smoking had higher CIMT than other patients. Mean of CIMT was found to be higher in HD patients with a history of CVD than that in patients without CVD history. Modi et al. [10] obtained similar results and confirmed our findings.
In our study, diabetes mellitus was one of the atherosclerosis accelerating factors, and these findings were similar to that in other studies, such as that of Modi et al.,[10] Tatsuyuki et al.,[11] and Abdelghaffar et al.[12]
Age and hemoglobin level in our study patients were similar to that in the studies by Modi et al.,[10] Irribaren et al.,[13] Tatsuyuk et al.,[11] and Dezitoeva et al.,[9] and had a positive significant relationship with CIMT. Similar to that in Abdelghaffar et al.'s study,[12] patients with BMI >25 had higher CIMT. High BMI is one of the accelerating factors of atherosclerosis in carotid arteries.
Whereas in the study patients a significant relationship was found between serum total cholesterol and CIMT of right carotid arteries, none was found with mean CIMT in both carotid arteries. Degoulet et al.[14] reported that lower total cholesterol had a significant relationship with mortality in HD patients. This controversial finding might be due to methodological characters. On the contrary, studies with cohort design and long-term follow-up must be performed for proper assessment of the relationship between total cholesterol and CIMT.
In our study and other similar studies, nutritional and inflammation states are two suspected confounding variables.[15] Iseki et al. carried out a retrospective study on HD patients with hypoalbuminemia; total cholesterol had a significant association with mortality.[16] Total cholesterol had a negative relationship with mortality in HD patients with high serum level of C-reactive protein (CRP), but in HD patients with low CRP level, total cholesterol had a positive significant relationship with mortality.[17] Studies on the assessment of temporal variations of serum level of albumin and cholesterol and also on their effects on survival of HD patients must be carried out in the future.
Conclusion
We show the prevalence and clinical correlates of subclinical atherosclerosis in Iranian dialysis patients. For more accurate results, we propose comparative studies for the assessment of sensitivity and specificity of ultrasonography for the diagnosis of coronary atherosclerosis in these patients.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Pathophysiology of vascular calcification in chronic kidney disease. Circ Res. 2004;95:560-7.
- [Google Scholar]
- Kidney disease as a risk factor for development of cardiovascular diseases: A statement from the American heart association councils on kidney in vascular disease, high pressure research, clinical cardiology, and Epidemiology and prevention. Circulation. 2003;108:2154-69.
- [Google Scholar]
- Intima-media thickness: A tool for atherosclerosis imaging and event prediction. Am J Cardiol. 2002;90:18L-21L.
- [Google Scholar]
- Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: The Atherosclerosis Risk in Communities (ARIC) Study, 1987–1993. Am J Epidemiol. 1997;146:483-94.
- [Google Scholar]
- Does renal failure cause an atherosclerotic milieu in patients with end-stage renal disease? Am J Med. 2001;110:198-204.
- [Google Scholar]
- Carotid intima-media thickness and plaques in hemodialysis patients. Artif Organs. 2000;24:691-5.
- [Google Scholar]
- Correlations between measures of atherosclerosis change using carotid ultrasonography and coronary angiography. Atherosclerosis. 2000;150:371-9.
- [Google Scholar]
- Carotid intima-media thickness and the risk of new vascular events in patients with manifest atherosclerotic disease: The SMART study. Eur Heart J. 2006;27:1971-8.
- [Google Scholar]
- Calcification of peripheral arteries in patients with terminal renal failure on programmed hemodialysis. Ter Arkh. 2005;77:50-4.
- [Google Scholar]
- Utility of carotid intimal medial thickness as a screening tool for evaluation of coronary artery disease in pre-transplant end stage renal disease. J Postgrad Med. 2006;52:266-70.
- [Google Scholar]
- The impact of visceral fat on multiple risk factors and carotid atherosclerosis in chronic haemodialysis patients. Nephrol Dial Transplant. 2003;18:1842-7.
- [Google Scholar]
- Carotid intima-media thickness: An index for subclinical atherosclerosis in type 1 diabetes. J Trop Pediatr. 2006;52:39-45.
- [Google Scholar]
- Correlates of uric acid and its association with asymptomatic carotid atherosclerosis: The ARIC Study. Atherosclerosis Risk in Communities. Ann Epidemiol. 1996;6:331-40.
- [Google Scholar]
- Mortality risk factors in patients treated by chronic hemodialysis. Report of the Diaphane collaborative study. Nephron. 1982;31:103-10.
- [Google Scholar]
- Lipid abnormalities in end stage renal disease. Nephrol Dial Transplant. 1998;13:45-9.
- [Google Scholar]
- Hypocholesterolemia is a significant predictor of death in a cohort of chronic hemodialysis patients. Kidney Int. 2002;61:1887-93.
- [Google Scholar]
- Association between cholesterol level and mortality in dialysis patients: Role of inflammation and malnutrition. JAMA. 2004;291:451-9.
- [Google Scholar]




