

Translate this page into:
Whole body calcification in a hemodialysis patient
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 38-year-old male presented with necrotic lesions on both feet. He has had chronic kidney disease (CKD) for 21 years and been receiving hemodialysis treatment for the last 10 years. He had undergone parathyroidectomy for severe secondary hyperparathyroidism. The parathormone (PTH) level had reduced to 1200 pg/ml after surgery from a pre-op value of 3500 pg/ml but gradually started to increase again. The patient underwent a second surgery for recurrent parathyroid adenoma. Since then he was managed with active Vitamin D until current presentation. The patient had thick black necrotic lesions on the toes compatible with nephrocalcinosis [Figure 1a]. Admission laboratory values were as follows: creatinine 4.9 mg/dl, calcium 8.1 mg/dl, phosphate: 4.3 mg/dl and PTH 5542 pg/ml. The patient was started on broad spectrum antibiotic therapy along with hyperbaric oxygen treatment. Lower extremity computed tomographic (CT) angiography, and thoracoabdominal CT showed widespread dystrophic paranchymal calcifications as well as extensive atherosclerotic lesions and vessel wall calcifications. Severe destructive osteoporosis was also notable in all scanned areas [Figure 1b–e].
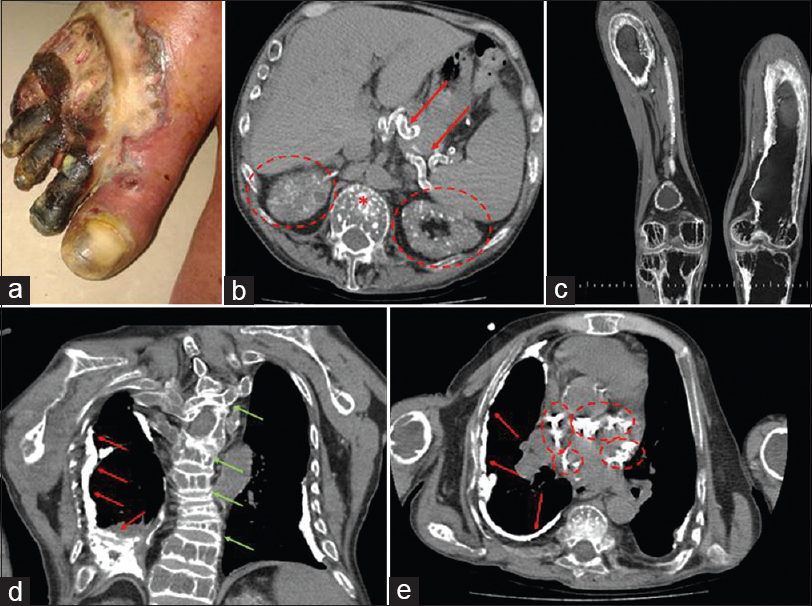
- (a) Deep ulcer with a diameter of 6 cm on dorsal aspect of the right foot, necrotic appearance in 2nd, 3rd, 4th and 5th fingers. (b) Extensive calcifications in mesenteric veins (arrows), calcium deposits compatible with nephrocalcinosis in both kidneys (ellipses) and severe osteopotic changes in the vertebrae (asterix). (c) Expansil growth due to Brown tumor and severe osteoporosis in bilateral femur and tibias seen in coronal reformatted images. (d) Pleural dystrophic calcifications in right pleural space (red arrows), compression fractures owing to severe osteoporosis and resultant scoliosis (green arrows). (e) Pleural dystrophic calcifications in right pleura in axial computed tomographic images (red arrows), widespread calcifications in coronary sinuses (veins) (ellipses)
Secondary hyperparathyroidism and bone and cardiac complications are now named as CKD-mineral and bone disorder (CKD-MBD).[1] When left untreated, CKD-MBD may have serious health consequences.[2] As in our case, sky-high serum PTH levels led to calcifications, osteoporosis and Brown tumors in the whole skeletal system, but more importantly in the vascular system and parenchymal organs throughout the body. Both surgical and medical treatment options were attempted in our patient, including surgery, active Vitamin D, oral phosphorus binders, efficient hemodialysis and cinacalcet. Unfortunately, some cases may be resistant to all these treatments.
This case illustrates dramatic changes secondary to severe and resistant secondary hyperparathyroidism and fortunately rarely encountered in this modern age of secondary hyperparathyroidism management.
Source of Support: Nil
Conflict of Interest: None declared.
References
- The new kidney disease: Improving global outcomes (KDIGO) guidelines – Expert clinical focus on bone and vascular calcification. In: Clin Nephrol. Vol 74. 2013. p. :423-32. [Erratum in: Clin Nephrol 2013;80:80]
- [Google Scholar]
- Kidney bone disease and mortality in CKD: Revisiting the role of Vitamin D, calcimimetics, alkaline phosphatase, and minerals. Kidney Int Suppl. 2010;117:S10-21.
- [Google Scholar]




