

Translate this page into:
Bilateral renal cortical necrosis in a patient undergoing in vitro fertilization
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Ovarian hyperstimulation syndrome (OHSS) due to cytokine release is a rare, iatrogenic complication of ovulation induction therapy in women undergoing in vitro fertilization (IVF). In severe cases, it can cause multiorgan dysfunction including acute kidney injury.[1]
A 28-year-old obese female with unexplained infertility, presented with a 4-day history of nausea, vomiting, abdominal distention, and generalized swelling. She had decreased urine output since the last 3 days and was anuric at presentation. She recently underwent ovulation induction in an IVF unit with clomiphene citrate 100 mg on days 2–6 of her menstrual cycle followed by injectable FSH on days 7–9 of the cycle. She received injectable human chorionic gonadotropin (hCG) 5000 IU 1-day before her symptoms.
On examination, she was conscious and oriented. She was in moderate respiratory distress with an oxygen saturation of 92% on 4 L/min of oxygen. Her blood pressure was 104/66 mm Hg, heart rate of 110/min, and respiratory rate of 26/min. Her neck veins were distended. Her abdomen was distended with a positive shifting dullness. The respiratory examination was significant for decreased air entry in bilateral lung fields. Chest X-ray was suggestive of bilateral pleural effusion. Abdominal ultrasound showed moderate ascites and enlarged ovaries (right ovary 46 × 32 mm and left ovary 61 × 35 mm) with multiple enlarged follicles.
Investigations showed elevated total count (28 × 103/µL), increased serum creatinine (6.5 mg/dl), elevated liver enzymes, hypoproteinemia with a low serum albumin level (2.2 g/l), and potassium level of more than 6 meq/L. Serum b-hCG was 8.7 mIU/l and serum estradiol 227.9 pmol/l. Repeated blood culture and urine culture did not grow any organism.
Based on her clinical, hematological, and biochemical parameters, a provisional diagnosis of severe OHSS with acute kidney injury was made. She was started on intravenous albumin infusion (20 g/100 ml), broad spectrum antibiotics, and initiated on hemodialysis. Over the next few days, her general condition improved, however, she continued to remain anuric. Further evaluation did not yield a cause for persistent renal failure. Antinuclear antibody, anti-dsDna, and antineutrophil cytoplasmic antibody (c-ANCA, p-ANCA) were negative. Antiphospholipid antibody syndrome was also negative (anticardiolipin, antiphospholipid, and antiglycoprotein antibody). A renal artery Doppler scan was within normal limits.
The kidney biopsy contained 42 glomeruli, all revealing global tuft necrosis along with necrosis of adjacent tubules and vasculature [Figure 1]. Tissue for immunofluorescence study included 11 glomeruli without a viable cortex. The renal biopsy was suggestive of a diffuse cortical necrosis. A contrast-enhanced computed tomography scan showed nonenhancing renal cortex, enhancing medulla, and no excretion of contrast medium, compatible with acute cortical necrosis.
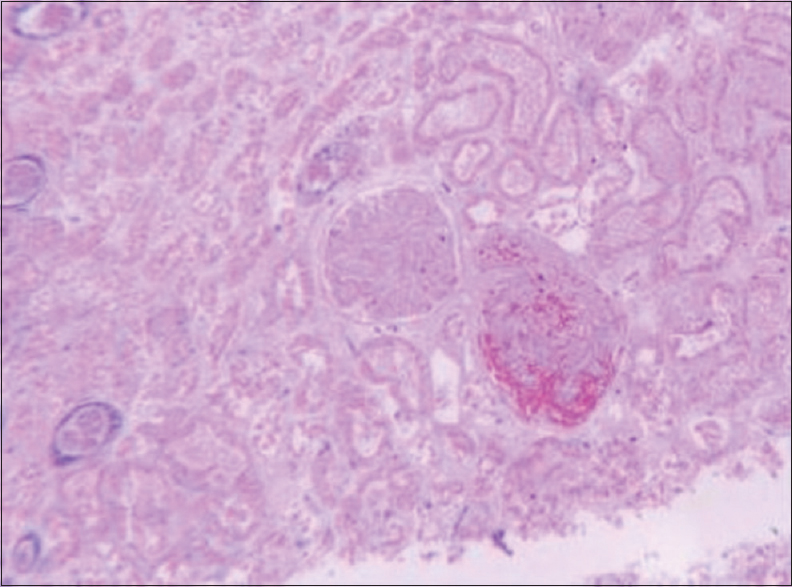
- Light microscopy showing complete necrosis of the glomerulus
Further course in the hospital was uneventful, and she was discharged a week later. Her urine output continued to remain <100 ml/day, and she was advised thrice a week hemodialysis.
The renal complications secondary to OHSS most commonly include prerenal AKI secondary to the massive fluid shift associated with increased vascular permeability. This, if left untreated, leads to ischemic damage to the kidney leading to acute tubular necrosis, which is frequently reversible.[2] There are few published case reports of compression of the distal ureters caused by massively enlarged ovaries resulting in obstructive uropathy. These were managed either by double-J stenting or placing percutaneous nephrostomies.[3] A case of nephrotic syndrome secondary to OHSS was also reported.[4]
Acute cortical necrosis, which is most commonly seen following obstetric complications, has never been reported with OHSS. The case highlights the need to recognize this entity as a potential complication of ovulation induction and requires close monitoring during ovarian stimulation and adherence to rigid guidelines and criteria for cancelling cycles.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Severe OHSS: An 'epidemic' of severe OHSS: A price we have to pay? Hum Reprod. 1999;14:2181-3.
- [Google Scholar]
- Ovarian hyperstimulation syndrome: Pathophysiology, staging, prediction and prevention. Ultrasound Obstet Gynecol. 2015;45:377-93.
- [Google Scholar]
- Obstructive uropathy as the etiology of renal failure in ovarian hyperstimulation syndrome. Fertil Steril. 2008;89:992.e1-2.
- [Google Scholar]
- Nephrotic sydrome developing in severe ovarian hyperstimulation syndrome. Int J Fertil Steril. 2014;7:345-8.
- [Google Scholar]




