

Translate this page into:
Ambulatory Blood Pressure Monitoring – Kids Need it Too?
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Ambulatory blood pressure monitoring (ABPM) has a well-established role in the management of hypertension in adults.[1] For the past decade, ABPM has been used effectively in children.
ABPM is performed using fully automated, lightweight machines programmed to measure blood pressure (BP) by oscillometric technique every 20–30 min. The ABPM machine is fitted along with an appropriate sized cuff in the clinic, after which the patient is allowed to return home to his routine activities. BP readings are obtained for a period of 24 h, during the day (awake BP) as well as the night (sleep BP). ABPM eliminates the white-coat effect and inter-observer bias (both weaknesses of measuring BP in the clinic) and allows assessment of diurnal BP variation. Once the 24 h monitoring period is complete, the BP readings are downloaded to a computer and edited to obtain the following BP indices:
-
Mean systolic and diastolic BPs during awake, sleep and 24 h periods. These are compared with clinic BPs
-
BP loads - the percentage of BP readings higher than the threshold values defining hypertension
-
Nocturnal dip - the percentage drop in mean BP from awake to sleep periods, normally >10%.
In adults, the threshold to define hypertension has been determined by studying a cohort of almost 6000 subjects for 10 years which yielded their cardiovascular, cardiac, and stroke outcomes based on measurement of ambulatory BP.[2] In pediatrics, the 95th percentile of BP values based on population-based distribution curves are used to define hypertension. This is because there is a very low incidence of actual cardiovascular events in the general pediatric population. Outcomes of hypertension may be preclinical (such as vessel wall damage and left ventricular hypertrophy) and therefore not routinely measured. The longitudinal data to link actual pediatric BP values (either auscultatory or by ABPM) for actual events like stroke and cardiac events is lacking.
In order to make the diagnosis of white coat hypertension or masked hypertension, data from ABPM is always interpreted along with a clinic BP measurement, preferably measured by auscultation.
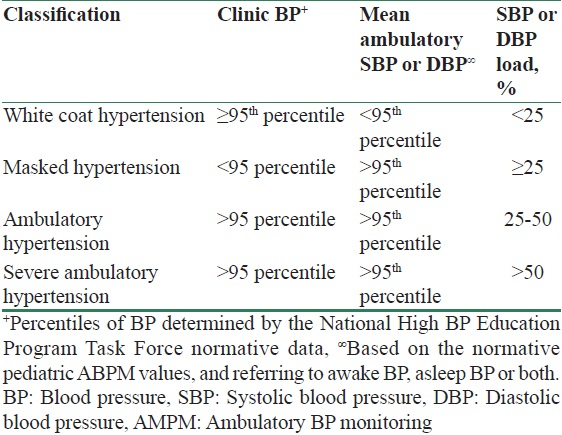
The American Heart Association has published guidelines [34] regarding the indications and interpretation of ambulatory BP data in children, with the following schema suggested for staging of ambulatory BP: Table 1.
In addition to making a diagnosis of white coat hypertension, ABPM is indicated in children with chronic kidney disease (CKD), renal transplant recipients, suspected secondary hypertension, and in genetic syndromes associated with hypertension for example, neurofibromatosis type 1 and Turner's syndrome. ABPM is also useful in evaluating the effectiveness of antihypertensive therapy, especially for those with nocturnal hypertension where clinic BPs may not detect elevated BPs.
Children with CKD are frequently hypertensive and at risk for cardiovascular morbidity.[56] In the CKD in children (CKiD) study, over 300 children underwent ABPM: greater than 50% had ambulatory hypertension, with “sleep hypertension” being more prevalent than “awake hypertension.” These children with masked hypertension would have remained undiagnosed by clinic BP measurements alone.[7] Children with higher BP loads have been shown to have lower glomerular filtration rate and a higher degree of proteinuria, compared to those with normal BP.[8] Strict BP control in children using ABPM is associated with a delay in progression of CKD.[9] In children with and without CKD, ABPM is a better predictor of target organ damage (left ventricular hypertrophy) than clinic BP.[10]
Home BP monitoring (HBPM) is performed using an oscillometric device. The mean of duplicate readings is taken twice daily for 7 days with data from the first day excluded. In pediatric CKD, HBPM was found to be superior to clinic BP but not as sensitive or specific as ABPM.[11] It must be remembered that oscillometric devices are available from various manufacturers that use different algorithms to calculate the systolic and diastolic BP from the measured mean BP. This lack of standardization might lead to lower reliability, especially when it comes to pediatric BP measurement. Ultimately, ABPM is the only modality that provides many BP measurements throughout different times of the day, especially the nighttime. Therefore, using ABPM one could diagnose nocturnal hypertension, study the diurnal variation of BP, assess the nocturnal dip and plan how best to time antihypertensive medications. Given the high rate of “sleep hypertension” in children with CKD and transplants, clinic BP and HBPM would underdiagnose such “masked hypertension.”
ABPM is cost-effective in all age groups. in an American study of 126 patients who received ABPM for initial evaluation of hypertension, the authors reported large savings upon the diagnosis of white coat hypertension.[12] Though data of cost-effectiveness of ABPM in India is lacking, we posit that it is indeed a highly cost-effective method of investigating and treating hypertension, especially in children. The identification of white coat hypertension saves the child from otherwise costly evaluation and unnecessary treatment. In children with CKD, ABPM leads to efficient prescribing of antihypertensive medications based on the diurnal variation of BP. More effective BP control, as determined by ABPM would lead to fewer hospitalizations and visits to the doctor for hypertension management. Furthermore, practically speaking, while the purchase of an ABPM machine with software requires a modest initial investment by the medical team, the cost to the patient can be made quite low. The ABPM would then be accessible to all, and in a center that manages pediatric hypertension, ABPM would be cost-effective in a relatively short period of time.
The use of ABPM in Indian children has been limited. In the first reported study of ABPM in children with CKD, the authors had successfully performed ABPM on 46 children.[13] Similar to the western literature, there was a high prevalence of ambulatory hypertension, up to 90% in children on dialysis. Nocturnal hypertension was especially prevalent. Of significance is the fact that although 74% of the study subjects were known to be hypertensive, ABPM revealed that almost half of them had inadequate BP control. The diagnosis of hypertension was missed in 7 out of 13 children with left ventricular hypertrophy when clinic BP alone was used to diagnose hypertension. ABPM subsequently detected hypertension in all these children.
Pediatric ABPM is not without limitations. The normative data defining hypertension has been generated from European children, and may not apply to our population. Furthermore, ABPM is difficult to perform in the very young (usually under 5 years of age) who may not comply with frequent BP readings. However, this study demonstrates that ABPM is not just feasible in the Indian setting, but also contributes significantly to the improved diagnosis and management of hypertension in children with CKD. Given the significant burden of morbidity associated with pediatric hypertension, one could argue that ABPM should be made the standard of care in pediatric CKD.
References
- European society of hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31:1731-68.
- [Google Scholar]
- International database on ambulatory blood pressure monitoring in relation to cardiovascular outcomes investigators. Diagnostic thresholds for ambulatory blood pressure monitoring based on 10-year cardiovascular risk. Circulation. 2007;24:2145-52.
- [Google Scholar]
- AHA scientific statement: Ambulatory blood pressure monitoring in children and adolescents: Recommendations for standard assessment. Hypertension. 2008;52:433-51.
- [Google Scholar]
- Update: ambulatory blood pressure monitoring in children and adolescents: a scientific statement from the American Heart Association. Hypertension. 2014;63:1116-35.
- [Google Scholar]
- Blood pressure in children with chronic kidney disease: a report from the chronic kidney disease in children study. Hypertension. 2008;52:631-7.
- [Google Scholar]
- Advanced coronary and carotid arteriopathy in young adults with childhood-onset chronic renal failure. Circulation. 2002;106:100-5.
- [Google Scholar]
- Ambulatory blood pressure patterns in children with chronic kidney disease. Hypertension. 2012;60:43-50.
- [Google Scholar]
- Strict blood-pressure control and progression of renal failure in children. N Engl J Med. 2009;361:1639-50.
- [Google Scholar]
- Ambulatory blood pressure and left ventricular mass index in hypertensive children. Hypertension. 2002;39:903-8.
- [Google Scholar]
- Masked hypertension associates with left ventricular hypertrophy in children with CKD. J Am Soc Nephrol. 2010;21:137-44.
- [Google Scholar]
- Escape Trial Group. Home, clinic, and ambulatory blood pressure monitoring in children with chronic renal failure. Pediatr Res. 2004;55:492-7.
- [Google Scholar]
- Cost-effectiveness of ambulatory blood pressure monitoring in the initial evaluation of hypertension in children. Pediatrics. 2008;122:1177-81.
- [Google Scholar]
- Role of 24-h ambulatory blood pressure monitoring in children with chronic kidney disease. Indian J Nephrol. 2015;25:355-61.
- [Google Scholar]




