

Translate this page into:
Unusual Case of Acute Lung Injury in a Renal Allograft Recipient
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
A renal allograft recipient developed cough with hemoptysis on the 1st postoperative day. A chest X-ray was performed which was suggestive of fluid overload. His fluid was restricted and diuretics were added. On the same day, his pulmonary infiltrates worsened and a computed tomography (CT) of the chest was carried out, which was suggestive of the right lower lobe consolidation and left pleural effusion. He underwent a bronchoscopy and the lavage was sent for cultures, which did not grow any infective organism. Besides routine antibiotics, treatment for possible cytomegalovirus, fungal infections, and pneumocystis infection was instituted. Noninvasive ventilation was started on day 8. A repeat CT of the chest on the postoperative day 8 showed further worsening of the pulmonary infiltrates. As all the initial cultures and serology were negative, a possibility of interstitial pneumonitis was considered. Mycophenolate sodium was considered as a possible cause of the lung infiltrates and was withdrawn. The patient showed progressive improvement. His antibiotics were withdrawn. He was discharged on day 14. A repeat CT 4 weeks post transplant showed significant improvement in his pulmonary pathology. The acute lung injury was considered to be a drug reaction secondary to mycophenolate sodium. In a renal allograft recipient with persistent pulmonary infiltrates, interstitial involvement secondary to drugs should be considered if the patient does not improve with the standard treatment measures.
Keywords
Mycophenolate sodium
pulmonary infiltrates
renal transplant

Introduction
Pulmonary infiltrates post renal transplant are usually secondary to volume overload or infections. Volume overload is usually secondary to an aggressive fluid resuscitation in a patient whose kidney function is still evolving. The commonest infection is usually bacterial in the immediate post transplant period. However in a small group of patients interstitial lung involvement can cause significant pulmonary involvement. We report a case of unusual pulmonary infiltrates which was thought to be secondary to mycophenolate sodium.
Case Report
A 46-year-old man presented to us with uremic symptoms in November 2014. He was evaluated and found to have end-stage kidney disease (native kidney disease of uncertain etiology) and was started on hemodialysis, with a temporary right internal jugular catheter and later with a left radiocephalic fistula upon maturation. His viral serology was negative.
He gave a history of long-standing hypertension and an ultrasound done 1 year back showed contracted kidneys. He was subsequently evaluated for transplantation and was found clinically fit for the same. Pretransplant cardiac assessment showed a normal ejection fraction echocardiographically, and a coronary angiogram on the advice of cardiologist showed complete occlusion of the right coronary artery. He was advised medical management for his coronary artery disease. His preanesthetic pulmonary evaluation did not reveal any abnormality.
In July 2015, after 7 months on dialysis, he underwent a living kidney transplantation (donor was his brother–in-law with a four antigen mismatch). The surgery was uneventful with no evidence of hemodynamic instability intraoperatively. He received 1 L of intravenous fluids during surgery and did not need any blood transfusion. The allograft attained immediate function. On the 1st postoperative day, his vitals were stable and he was diuresing well with a total urine output of more than 5 L. There was no clinical evidence of fluid overload.
He received basiliximab as induction with tacrolimus, mycophenolate sodium, and steroids as his maintenance immunosuppression. The tacrolimus (0.1 mg/kg/day in two divided doses) and mycophenolate sodium (720 mg twice a day) was started 48 h before the transplantation surgery. On the same day, he developed cough with breathlessness. The chest X-ray was suggestive of pulmonary edema, and consequently, he was started on diuretics, and his fluid intake was restricted. His central venous pressure was 11 cm of water, and his electrocardiogram and echocardiogram did not show any fresh changes. The serum Troponin levels were normal. His respiratory condition continued to worsen and a computed tomography (CT) scan of the chest was done which showed patchy right lower lobe consolidation, bilateral ground-glass densities with minimal left pleural effusion [Figure 1]. Cultures for bacteriological, mycobacterial, and fungal isolation were sent and antibiotics were started. His total counts were normal and the calculated eosinophil count was <100 cells/μL. His procalcitonin levels were normal. His antibiotics were upgraded and a pulmonary consult was asked for. The pulmonologist opinion was that of noncardiogenic pulmonary edema, and he suggested continuation of diuretics. Despite adequate diuresis and antibiotics, his oxygen saturation continued to deteriorate. Besides antibiotics, treatment for possible fungal, cytomegaloviral, and pneumocystis infection was started and bronchoscopy was done. Initial bronchoalveolar lavage evaluation and cultures came negative for all infective pathology. All anti-infectives except antibiotics were withdrawn.
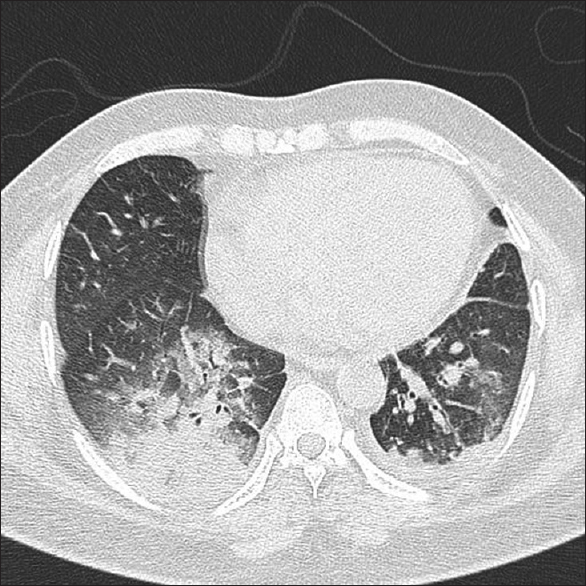
- Initial computed tomography done on the 1st postoperative day showing right lower lobe consolidation and left pleural effusion
Because of his persistent pulmonary infiltrates, the second dose of basiliximab (day 4) was not given. On the 8th postoperative day in view of his worsening clinical condition, he was put on noninvasive ventilation and a repeat CT scan of the chest was done. The CT scan showed confluent ground-glass densities in both the lungs with smooth interlobar septal thickening. Certain parts of the parenchyma were spared giving a crazy pavement pattern [Figure 2a and b]. As there was no radiological evidence of infection and fluid overload, a diagnosis of interstitial pneumonitis was considered. A drug-induced etiology of the lung pathology was considered secondary to mycophenolate sodium (idiosyncratic reaction as there was no skin rash, arthralgia, or blood eosinophilia) and the drug was withdrawn. Over the next 4 days, he showed progressive improvement. His oxygen requirement came down dramatically, and he was discharged on day 14 in stable clinical condition without any oxygen requirement. A repeat CT scan of the chest after 4 weeks showed considerable improvement in the pulmonary infiltrates. [Figure 3a and b] The patient is doing well after 6 months posttransplantation.

- (a) Confluent ground-glass densities in both the lungs noted in the computed tomography scan done on the 8th postoperative day. (b) Extensive pulmonary infiltrates in the coronal images

- (a) Near total resolution of pulmonary infiltrates on follow-up after 4 weeks. (b) Coronal images showing radiological improvement on follow-up
Discussion
Pulmonary infiltrates presenting in a renal allograft recipient early in the course of transplant is often considered to be a pulmonary infection and early antibiotics are started.[1] Even though the incidence of bacterial pneumoniae is decreasing, multidrug-resistant bacteria are emerging as growing threat.[2] Some reports have revealed that the use of newer immunosuppressive medications (tacrolimus, mycophenolate mofetil, induction therapy) and inappropriate use of antibiotics have led to an increased rates of bacterial pulmonary infection.[3] Some studies have shown that consistent use of antiviral/antifungal prophylaxis reduces the incidence of cytomegalovirus and pneumocystis infections.[4] However, there are other studies which have shown an increasing trend of fungal infection in renal allograft recipients, which is a major cause of posttransplant mortality.[5] In many instances, the bacterial pathogen remains unidentified. In our patient also, the early sputum and bronchial lavage did not yield any organism and he was treated empirically with broad-spectrum antibiotics. Antifungal and antiviral therapy was subsequently added as his pulmonary infiltrates continued to deteriorate.
One of the major issues to be considered in the differential diagnosis of worsening pulmonary infiltrates in a renal allograft recipient is to consider noninfectious causes of the pulmonary pathology.[6] Pulmonary edema, pulmonary hemorrhage, and interstitial pneumonitis are seen in renal allograft recipients and should be part of the differential diagnoses of pulmonary infiltrates in renal transplant recipients.
Interstitial pneumonitis, especially secondary to drugs, has been reported in literature. There are several reports regarding target of rapamycin inhibitors and interstitial lung disease, following kidney transplantation.[7] Though rare, there are a few reports of pulmonary toxicity secondary to the use of azathioprine [8] and mycophenolate mofetil.[9] In our patient, drug-induced interstitial pneumonitis was considered and mycophenolate sodiumwas withdrawn. The dramatic improvement in the pulmonary infiltrates following withdrawal of mycophenolate sodium led us to believe that mycophenolate sodium was the cause of the lung infiltrates in our patient.
Mycophenolate sodium is a morpholinoethyester of mycophenolic acid. It acts as an inhibitor of inosine monophosphate dehydrogenase isoform 2 and selectively inhibits T and B lymphocytes and is effective in preventing early acute rejection.[10] It has become the most common immunosuppressive agent used in solid organ transplantation.[11] The major side effects of the drug are predominantly gastrointestinal and hematologic. Very little information regarding pulmonary toxicity exists in literature and it is unclear whether pulmonary toxicity occurs along with other known side effects or it manifests as a solitary phenomenon. Some studies have shown that there is an association between the drug level and side effects of the drug, but the clinical benefit of drug level monitoring is still of questionable value in such situation where the adverse effect is considered to be an idiosyncratic reaction.[11] Drug level monitoring in our patient was not done because of lack of facility. The toxicity of mycophenolate mofetil was considered to be idiosyncratic in our patient.
Our patient is currently doing well. He has normal renal functions and no respiratory signs and symptoms. The patient is currently on steroids and tacrolimus.
Conclusion
In a patient with worsening pulmonary infiltrates, which cannot be related to infections and fluid overload, consideration should be given to interstitial lung injury. Drugs are known to cause interstitial lung injury, and immunosuppressive agents are being recognized as potential causes for persistent pulmonary pathology in a solid organ recipient.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest. No added information as the authors have not received any honorarium from any pharmaceutical company.
References
- Respiratory infection in the AIDS and immunocompromised patient. Eur Radiol. 2004;14(Suppl 3):E21-33.
- [Google Scholar]
- Pulmonary complications in renal recipients after transplantation. Transplant Proc. 2011;43:551-3.
- [Google Scholar]
- Pulmonary infiltrates in the non HIV- infected immunocompromised patient: Etiologies, diagnostic strategies and outcomes. Chest. 2004;125:260-71.
- [Google Scholar]
- Pulmonary infections after kidney transplantation. J Assoc Physicians India. 1999;47:779-83.
- [Google Scholar]
- Pulmonary fungal infections in kidney transplant recipients: An 8-year study. Transplant Proc. 2009;41:1654-6.
- [Google Scholar]
- Noninfectious pulmonary complications of liver, heart, and kidney transplantation. Clin Chest Med. 2005;26:623-9, vii.
- [Google Scholar]
- Sirolimus-induced pneumonitis after renal transplantation: A single-center experience. Transplant Proc. 2012;44:161-3.
- [Google Scholar]
- Severe pulmonary toxicity after azathioprine/6-mercaptopurine initiation for the treatment of inflammatory bowel disease. J Clin Gastroenterol. 2007;41:682-8.
- [Google Scholar]
- Acute respiratory failure and pulmonary fibrosis secondary to administration of mycophenolate mofetil. Transplantation. 1997;64:1607-9.
- [Google Scholar]
- Lymphocyte-selective cytostatic and immunosuppressive effects of mycophenolic acid in vitro: Role of deoxyguanosine nucleotide depletion. Scand J Immunol. 1991;33:161-73.
- [Google Scholar]
- Therapeutic monitoring of mycophenolate mofetil. Clin J Am Soc Nephrol. 2007;2:184-91.
- [Google Scholar]




