

Translate this page into:
Lumps All Over: A Case of Chronic Tophaceous Gout (Harrison Syndrome)
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 65-year-old male, resident of Mumbai was referred to Bombay Hospital Institute of Medical Sciences in August 2012, with a history of multiple painless lumps. The patient was a known diabetic, hypertensive, and a case of chronic kidney disease for 10 years and on maintenance dialysis for 5 years. He had a history of episodic podagra relieved by over-the-counter medications. He was noncompliant to his medications which included a xanthine oxidase inhibitor. Since 6 months, he noticed multiple yellow-white painless subcutaneous deposits initially noticed over small joints of hands [Figure 1] and toes [Figure 2a] but later also around elbow [Figure 2b] and knee joints. His serum uric acid levels were elevated 14.6 mg/dl (normal 2.6–6.8 mg/dl). His X-rays revealed chalky white periarticular calcifications over small joints of the hands [Figure 3a], ankle joint [Figure 3b], and knee joint [Figure 3c]. Examination revealed weeping serosanguinous fluid with a milky-white discharge from the second toe of his left leg. Examination of the fluid showed monosodium urate (MSU) crystals with apple-green birefringence. He underwent debridement of the wound and was discharged on an oral xanthine-oxidase inhibitor (febuxostat 80 mg). Six weeks later, his uric acid levels normalized to 5.6 mg/dl. He denied any surgical treatment.
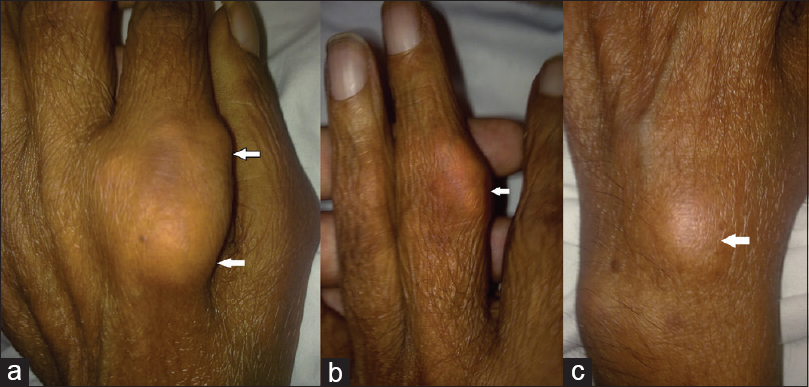
- (a) Left panel – massive tophus over second metacarpophalangeal joint, (b) middle panel – big tophus overlying proximal interphalangeal joint, (c) right panel – tophus overling dorsum of the left hand (pointed by horizontal arrows)

- (a) Right panel – tophi overlying extensor compartment of the right forearm, (b) Left panel – multiple yellow-white tophi over first metatarsophalangeal joint (pointed by arrow) and over medial malleolus (pointed by arrowheads)

- (a) Left panel – soft tissue calcific deposit over the left middle proximal interphalangeal joint (pointed by arrow) and at distal second metacarpal of the right hand (pointed by arrowhead), (b) middle panel – chalky white calcific deposits behind the right fibula (arrow) and diffuse subcutaneous collection of deposits (arrowheads), (c) right panel – calcific deposit overlying lateral side of the left knee joint (arrow)
Gout is a common metabolic disease caused by deposition of MSU crystals in peripheral joints. Tophi are formed by nodular accumulation of MSU crystals in soft tissue that usually appears in the metatarsophalangeal joint or knee. However, tophi in the hands are not common.[1] Similarly, large tophi are unusual in chronic gout.[2] Tophi are usually present in patients who have had gouty arthritis for at least 10 years.[1] Tophus is the cardinal feature of advanced gout. Microscopically, tophi are chronic foreign body granuloma-like structures containing collections of MSU crystals surrounded by inflammatory cells and connective tissue.[3] The primary therapy is treatment with antihyperuricemic drugs. Surgical removal of tophi is also reported to reduce pain, maximize function, and improve cosmesis.[1]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Giant gouty tophi in the hands. Lancet Diabetes Endocrinol 2016 Feb 19:pii: S2213-8587(15) 00420-9. doi: 10.1016/S2213-8587(15) 00420-9. [Epub ahead of print] PubMed PMID: 26907672
- [Google Scholar]
- Chronic tophaceous gout with unusual large tophi: Case report. Pan Afr Med J. 2015;22:132.
- [Google Scholar]




