

Translate this page into:
Association of Amelogenesis Imperfecta and Bartter's Syndrome
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Bartter's syndrome is an autosomal recessive renal tubular disorder characterized by hypokalemia, hypochloremia, metabolic alkalosis, and hyperreninemia with normal blood pressure. Bartter's syndrome is associated with hypercalciuria and nephrocalcinosis. Amelogenesis imperfecta (AI) is a group of hereditary disorders that affect dental enamel. AI could be part of several syndromes. The enamel renal syndrome is the association of AI and nephrocalcinosis. We report two patients of AI with Bartter's syndrome.
Keywords
Amelogenesis imperfecta
Bartter's syndrome
nephrocalcinosis
yellow teeth

Introduction
Bartter's syndrome is an autosomal recessive renal tubular disorder characterized by hypokalemia, hypochloremia, metabolic alkalosis, and hyperreninemia with normal blood pressure. The underlying renal abnormality results in excessive urinary losses of sodium, chloride, and potassium. Amelogenesis imperfecta (AI) is a group of hereditary disorders that affect dental enamel.[1] It might affect all or some teeth in the deciduous and/or permanent dentition. AI has been reported as an isolated or syndromic finding with an autosomal dominant, autosomal recessive, or X-linked inheritance. AI could be part of syndromes in association with amelo-onycho-hypohidrotic syndrome, Kohlschutter syndrome, oculo-dento-osseous dysplasia, and epidermolysis bullosa hereditaria.[23] The rare syndrome associating AI and nephrocalcinosis, also called enamel renal syndrome, was first reported by MacGibbon in 1972.[4] A previous study reported two patients of AI in association with Bartter's syndrome.[5] We report two patients of AI with Bartter's syndrome.
Case Reports
Patient 1
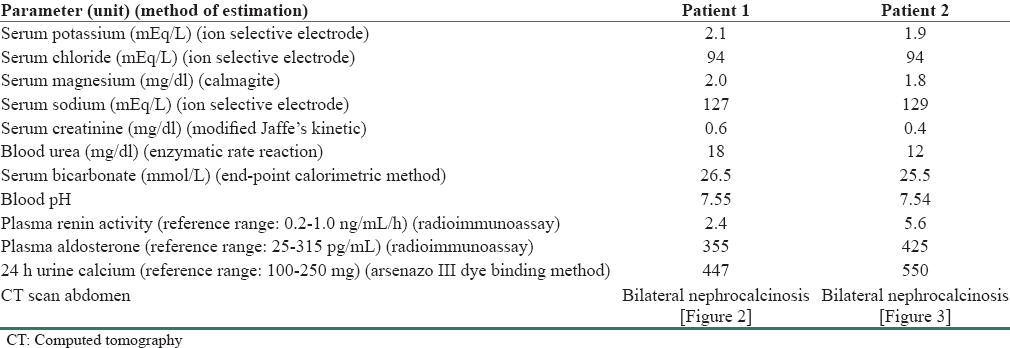
A 12-year-old boy presented with sudden onset weakness of both upper and lower limbs. He had history of polydipsia, increased frequency of urination, fatigue and muscle weakness of week duration. There was no history of recurrent carpopedal spasms. The boy had a previous episode of sudden onset weakness of both upper and lower limbs about 4 months ago. His parents' marriage was nonconsanguineous. There was no history of maternal polyhydramnios or premature delivery. There was no history of failure to thrive, salt craving, vomiting, and constipation. He had normal developmental milestones. However, the scholastic performance of boy was poor. Blood pressure was 90/60 mmHg. Height was 138 cm. Weight was 29 kg. Oral cavity examination revealed yellowish teeth [Figure 1] presenting rough surfaces and conspicuous and irregular defects. The enamel alterations were generalized, affecting teeth in both arches. The gingivae were without signs of inflammation. The systemic examination was unremarkable. The investigations are given in Table 1.

- Amelogenesis imperfecta of patient 1
Patient 2
A 13-year-old girl presented with sudden onset weakness of both upper and lower limbs. She had history of polydipsia and increased frequency of urination. There were other symptoms also such as fatigue, muscle weakness, cramps, and recurrent carpopedal spasms. There was no similar history in the past. Her parents' marriage was nonconsanguineous. There was no history of maternal polyhydramnios or premature delivery. There was no history of failure to thrive, salt craving, vomiting, and constipation. She had normal developmental milestones. The scholastic performance of the girl was optimum. Blood pressure was 80/60 mmHg. Height was 136 cm. Weight was 30 kg. Oral cavity examination revealed yellowish teeth [Figure 4]. The surfaces were rough and irregular. The gingivae were without signs of inflammation. The systemic examination was unremarkable. The investigations are given in Table 1.

- Bilateral nephrocalcinosis of patient 1
- Bilateral nephrocalcinosis of patient 2

- Amelogenesis imperfecta of patient 2
Both the patients were treated with potassium chlorate supplement and spironolactone 12.5 mg twice a day. There were no symptoms in next 1 year of follow-up.
Discussion
Dental enamel is the most mineralized tissue in the human body. More than 95% of mature enamel is mineral. The organic content is <1%.[6] The dentin matrix is secreted initially by odontoblasts. It is followed by the secretion of the enamel matrix by ameloblasts.[7] The enamel matrix is subsequently calcified and matured across the removal of remaining enamel matrix proteins and by the growth of the enamel crystallites. Alterations in any of these steps induce development of enamel defects.[7] Enamel malformation might result in dental enamel defects such as discoloration of teeth, thin and/or smooth tooth enamel, and easily damaged teeth.[17] The association of AI and nephrocalcinosis was reported before.[28]
Bartter's syndrome is associated with hypercalciuria and nephrocalcinosis. In the thick ascending limb of the loop of Henle, 20% of the filtered calcium is reabsorbed largely by the cortical thick ascending limb, through both transcellular and paracellular routes. The apical Na+-K+-2Cl− cotransporter NKCC2 and the renal outer medullary potassium K+ (ROMK) channel generate a lumen-positive transepithelial potential difference, a “driving force” for paracellular cation transport. Chloride channel Kb (CLC-Kb) mediates Cl− exit through the basolateral membrane.[9] In Bartter's syndrome Types I, II, and III, NKCC2 cotransporter, ROMK channels, and CLC-Kb are abnormal proteins, leading to hypercalciuria and nephrocalcinosis. All patients of AI are not associated with Bartter's syndrome and vice versa.[5] Although a clear-cut familial association was not described, a previously described patient was born to consanguineous parents and had a possibility of Bartter's syndrome in that patient's older sister.[5] The development of nephrocalcinosis will depend on tubular delivery of calcium to the interstitium, as well as prevailing local conditions, including pH, inhibitory proteins, and anion concentrations.[10] The connection between Bartter's syndrome and AI is far more complex than only being a direct result of nephrocalcinosis and/or hypercalciuria. Therefore, the molecular mechanisms of calcium transport in renal tubules and dental tissues are to be further understood to learn the link between Bartter's syndrome and defects in enamel formation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: Problems in classification. J Oral Pathol. 1988;17:547-53.
- [Google Scholar]
- Amelogenesis imperfecta and nephrocalcinosis syndrome: A case report and review of the literature. Nephron Physiol. 2011;118:62-5.
- [Google Scholar]
- Case reports of a new syndrome associating gingival fibromatosis and dental abnormalities in a consanguineous family. J Periodontol. 2008;79:1287-96.
- [Google Scholar]
- Typical features of amelogenesis Imperfecta in two patients with Bartter's syndrome. Nephron Extra. 2012;2:319-25.
- [Google Scholar]
- Epithelial-mesenchymal signalling regulating tooth morphogenesis. J Cell Sci. 2003;116:1647-8.
- [Google Scholar]
- Amelogenesis imperfecta and nephrocalcinosis syndrome. Indian J Nephrol. 2014;24:260-1.
- [Google Scholar]
- Renal control of calcium, phosphate, and magnesium homeostasis. Clin J Am Soc Nephrol. 2015;10:1257-72.
- [Google Scholar]
- Nephrocalcinosis: Molecular insights into calcium precipitation within the kidney. Clin Sci (Lond). 2004;106:549-61.
- [Google Scholar]




