

Translate this page into:
Protective Effect of Gastric Distension Preconditioning on Renal Ischemia/Reperfusion Injury in Rats
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The stomach mechanoreceptors can be stimulated by gastric distension (GD) and through afferent vagal nerve, increased activity of the renal sympathetic pathways. Because renal sympathectomy can abolish the protective effect of ischemic preconditioning, it seems that GD preconditioning can be effective in renal ischemia/reperfusion (I/R) injury. Gastric inflate (8 ml of 37°C water for 20 min) by a latex balloon inserted into the stomach through the fundus; I/R group was subjected to 45 min of bilateral ischemia and 24 h of reperfusion. GD preconditioning decreases blood urea nitrogen, creatinine, kidney damage score, and alkaline phosphatase levels compared to the sham GD group (P < 0.05). GD preconditioning may protect renal I/R injury through anti-inflammatory activity, but this efficacy requires extensive studies on the methods and mechanisms.
Keywords
Gastric distension
ischemia/reperfusion
preconditioning
renal

Introduction
Ischemia/reperfusion (I/R) is a process that occurs in conditions such as septic shock, kidney transplant, or cardiovascular surgery and is a major cause of acute kidney injury (AKI) with a high mortality rate.[123] Increased renal sympathetic activity and subsequent related effects can be one of the factors involved in AKI caused by renal I/R.[4] Preconditioning is a procedure, by which deleterious subthreshold stimuli to tissue induce tolerance and resistance to the next stimulation in same or other kind of noxious stimuli.[5] Preconditioning of tissue may be created by different stimuli such as ischemic preconditioning (repetitive short periods of I/R),[6] hypoxia,[78] oxidative stress,[9] heat stress,[10] pharmacological agents,[1112] and lipopolysaccharides.[13] There is evidence that adenosine receptors, nitric oxide (NO), and sympathoexcitatory process involved in preconditioning mechanisms.[1415] Approximately 80%–90% of visceral sensory information is continuously transmitted to the nucleus tractus solitarius and area postrema of the brain stem by afferent vagus fibers.[16] This afferent impulse can initiate different peripheral reflexes including cardiovascular reflexes through sympathetic efferent pathways. It is known that part of the therapeutic effects of renal ischemic preconditioning is applied by the sympathetic nervous system and renal sympathetic denervation abolishes these effects.[15]
The stomach wall contains two types of mechanoreceptors, stretch and tension receptors which stimulate after mechanical stimuli of the stomach wall, such as distension or an increase in muscle tension that activate gastric vagal mechanosensitive afferents and relay information to the central nervous system.[1718] Efferent sympathoexcitatory responses can lead to hemodynamic changes such as increased arterial pressure and heart rate and peripheral vascular resistance.[1920]
Several evidence of possible positive effects of gastric distension (GD) preconditioning encourage us to evaluate its role for the first time on renal I/R injury.
Materials and Methods
Animals
Male Wistar rats (200–260 g) were maintained under standardized conditions 12 h light/dark cycle at a room temperature of 23°C ± 2°C.
Tap water and chow were freely available throughout the acclimatization and study periods. Animals were randomly divided into four groups: I/R, sham-operated I/R, GD before I/R, and sham-operated GD groups (7–8 in each).
Experimental methods
Before experimentation, animals were deprived of food for 16 h but allowed free access to water. The rats were anesthetized with 10% chloral hydrate through intraperitoneal injection. Renal I/R was induced as described previously.[21] Briefly, kidneys were excited through two flank incisions and renal pedicles with arteries and veins clamped for 45 min followed by 24 h of reperfusion. Occlusion and reperfusion arteries were verified visually by turned the color of kidneys from dark purple into red.
Sham-operated renal ischemia were identical surgical procedures of renal I/R except of renal arteries clamping.
Gastric distention was performed by a 2 cm length latex balloon that was attached to a polyethylene tube (1 mm diameter) and inserted into the stomach through a small incision in the fundus. A 10 ml syringe was attached to the cannula to inflate (8 ml for 20 min) (the physiological average of rat stomach capacity)[222324] and deflate the balloon with 37°C water. In sham-operated GD group, the same surgical procedure was applied without balloon inflation. Twenty-four hours after reperfusion under anesthesia, blood samples were drawn from the heart; then rats were killed by injection of KCl 10% into the heart, and plasma samples were extracted immediately and stored at −20°C until being assayed. The kidneys were excited and weighted, the right kidney homogenized and centrifuged at 6000 g for 10 min, and supernatant was centrifuged again at 15,000 g for 2 min. The left kidney was kept and fixed in 10% formalin solution for histological analysis. All rats' body weight (BW) was measured at the beginning of the experiments and before sacrifice.
Histological assessment
Dehydrated and paraffin-embedded renal tissues were sliced into 4 μm thick sections and stained with hematoxylin and eosin. Histological tubular necrosis was graded by light microscopy on a scale of 0–4 as follows:[25] 0 = normal kidney; 1 = minimal damage (<5% involvement of the cortex or outer medulla); 2 = mild damage (5%–25% involvement of the cortex or outer medulla); 3 = moderate damage (25%–75% involvement of the cortex or outer medulla); and 4 = severe damage (>75% involvement of the cortex or outer medulla).
Laboratory analysis
Serum levels of liver enzymes (alkaline phosphatase [ALP], aspartate aminotransferase [AST], and alanine aminotransferase [ALT]), urea, and creatinine were measured by autoanalyzer (Pars Azmun, Iran). Serum nitrite levels were determined using Nitrite Colorimetric Assay Kit (Promega Corporation, USA).
Serum and kidney supernatant levels of malondialdehyde (MDA) or concentration of thiobarbituric acid reactive substance was calculated from the absorbance at 532 nm; briefly, 500 μL of each sample was mixed with 10% trichloroacetic acid and centrifuged at 2000 g for 10 min and 500 μL of supernatant was added to 500 μL of 0/67% thiobarbituric acid and incubated in warm water bath for 10 min.
Statistical analysis
Data were expressed as mean ± standard error of the mean. Mean differences between groups were analyzed by the t-test and one-way analysis of variance. Pathological damage scores between the groups were compared by Mann–Whitney test and differences were considered significantly at P < 0.05.
Results
Assessment of renal function
Figure 1 shows the effect of GD and I/R on serum levels of blood urea nitrogen (BUN) (a) and creatinine (b) compared to sham GD and sham I/R groups. Forty-five minutes ischemia followed by 24 h reperfusion associated with significantly increased markers of renal function. Serum BUN levels increased significantly in I/R group compared to sham I/R from 22.36 to 66.99 mg/dl and decreased in GD group from the sham GD value of 58.41 to 39.45 mg/dl. Serum creatinine is reduced significantly by GD from 1.54 value in sham GD to 0.64 mg/dl and increased by I/R from 0.51 in sham I/R to 0.99 value.
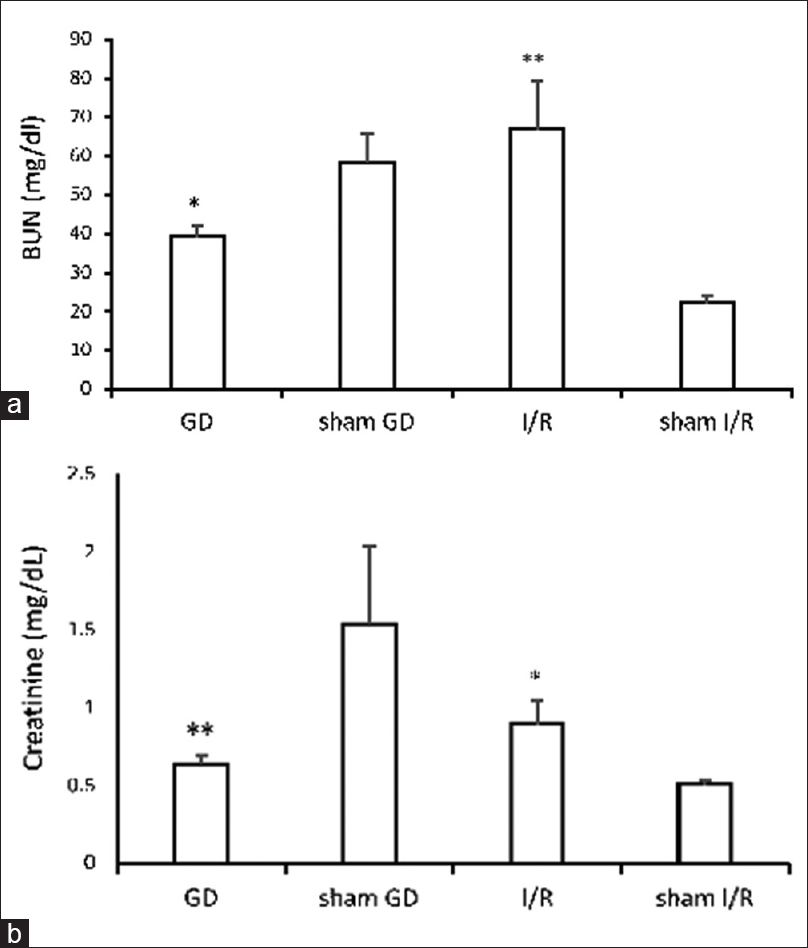
- Changes in serum blood urea nitrogen (a) and creatinine (b) levels in different groups: Gastric distension, sham gastric distension, ischemia/reperfusion, and sham ischemia/reperfusion. Values are the mean ± standard error of the mean. *P < 0.05 and **P < 0.01 are significantly different from the sham-related groups
Body and kidney weight
BW changes are shown in Figure 2a. As we see BW has no significant changes in groups. The kidney weight (KW)/100 g BW ratio as expected was significantly higher in I/R injury rats than in sham group [Figure 2b].
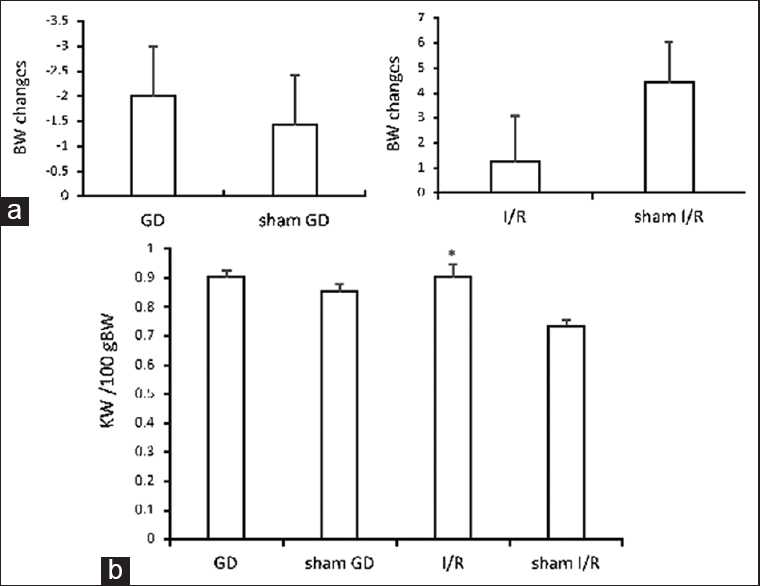
- Effect of gastric distension and ischemia/reperfusion-induced changes in body weight (a) and kidney weight/100 g body weight ratio (b). Data are means ± standard error of the mean (*P < 0.05 vs. sham ischemia/reperfusion)
Assessment of liver enzymatic function
Analysis of liver enzymatic levels revealed a lower significant difference of serum ALT and AST levels in the sham I/R than the I/R group and lower level of ALP in GD versus sham GD group [Figure 3a-c].

- Serum alanine aminotransferase (a) aspartate aminotransferase (b) and alkaline phosphatase (c) changes in gastric distension and ischemia/reperfusion groups compared to sham groups. All values are expressed as mean ± standard error of the mean. *P < 0.05 and **P < 0.01 were considered significant difference versus sham groups
Lipid peroxidation and free radicals assessment
The effect of I/R injury on lipid peroxidation and an increase in free radicals were evaluated by serum levels of MDA. There was an increase of MDA levels in I/R respect to the sham-operated group [Figure 4]. In this figure, there was an interesting data that serum MDA levels of sham GD with I/R were equal or even lower than sham I/R group with no I/R.

- Serum malondialdehyde levels change following ischemia/reperfusion injury, gastric distension, sham gastric distension, and sham ischemia/reperfusion rats. Data are presented as mean ± standard error of the mean (*P < 0.05 vs. sham-operated ischemia/reperfusion rats)
Histological results
Tubular injury and necrosis in GD and sham I/R rats was significantly less compared with that observed in kidneys from I/R and sham GD rats [Figure 5a]. Morphological studies using electron microscopy revealed histological kidney tubular damage in I/R and sham GD compared to sham I/R and GD rats, respectively [Figure 5b].

- Tubular injury score in the different groups. *P < 0.05 and ***P < 0.001 respect to sham-related group (a). Microscopic appearance of glomeruli and tubules and tubular necrosis from the gastric distension, sham gastric distension, ischemia/reperfusion, and sham ischemia/reperfusion groups (H and E, ×400) (b)
Kidney and serum nitrite levels assessment
As shown in Figure 6, there was no significant difference in kidney and serum nitrite levels between different groups.

- Serum and kidney nitrite levels of gastric distension, sham gastric distension, ischemia/reperfusion, and sham ischemia/reperfusion groups
Discussion
In this study, stomach balloon distension was used as a method to selectively activate gastric mechanoreceptors and vagal afferent neuron stimulation. To reflect the GD associated with the ingestion of a large meal, the balloon was inflated approximately the same mean volume of stomach filling in rats after an overnight fasting.[2223] For the first time, we showed that gastric stretch mechanoreceptors stimulation by GD preconditioning protects kidney from I/R-induced injury. Many investigations have indicated that ischemic preconditioning can reduce serum creatinine, BUN, and histological renal damage after renal I/R injury.[26] In this study, serum BUN and creatinine levels that commonly have been measured as evaluation markers of renal and glomerular function showed a significant decrease in GD group relative to sham-operated rats which indicates improving renal functions after GD preconditioning. Histological analysis also confirms beneficial effects of GD preconditioning on tissue injuries and cell death. The high KW/BW ratio is a measure of renal proliferation and hypertrophy, which have been observed in models of I/R.[27] As it is shown, KW/BW is higher in I/R whereas it did not change in GD compared to sham group. Increased liver enzymatic levels can be a warning of systemic inflammation diseases.[28] It is clear from the liver enzyme assays that GD is significantly associated with decrease in systemic inflammatory marker of ALP.[2930] ALP levels increase in patients with chronic kidney disease[31] and change in serum ALP levels may be a marker of identifying kidney dysfunction or an indicator of improved treatment.[32] Because inflammation plays an important role in the pathogenesis of renal I/R,[3] we suggest that therapeutic effects of GD preconditioning can be mediated through its anti-inflammatory activities.
Renal ischemia is the primary event leading to increased activity of the sympathetic nervous system which plays an important role in the development of I/R-induced acute renal failure.[433] Although we did not examine the effects of renal sympathetic activity, there are evidence that some parts of ischemic preconditioning treatments are due to sympathetic nervous system because sympathectomy eliminates preconditioning treatment effects.[15] The exact mechanism of ischemic preconditioning is not completely known but can be due of altered blood flow and some mediators such as NO and adenosine. Muscle layers of the stomach including mechanoreceptors that are stimulated by GD and causing hemodynamic responses through sympathetic efferent nerves.[1934] Some studies have showed the role of NO on ischemia preconditioning.[3536] Although in this study, GD has increased serum nitrite levels compared to the sham-operated group, this value was not statistically significant which may due to increased sympathetic nervous system activity that prevented of further nitrite levels following stomach mechanoreceptors stimulation.[33373839] MDA, as a marker of lipid oxidation, caused by free radicals reactions on cell membrane polyunsaturated fatty acids and its measurement can achieve information about oxidative stress in cells.[40] Interestingly, although there was no significant difference between serum MDA levels of GD and sham-operated GD rats, MDA levels in GD with renal I/R were the same as the sham I/R rats with no I/R and even significantly lower than I/R group. This result suggests that the stimulation of gastric mucosa with or without distension can reduce I/R-induced increased lipid peroxidation marker (MDA) to a value approximately normal levels.
Conclusions
This is the first study on the effect of GD as a nonischemic preconditioning on renal I/R injury. Before this renal nonischemic preconditioning can be used in clinical renal I/R, situations such as transplantation require more studies of the methods' effectiveness and extensive mechanisms.
Financial support and sponsorship
This study was funded by the Isfahan University of Medical Sciences. This study was funded by Isfahan University of Medical Sciences. Grant No. 194128.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
This study was supported by Isfahan University of Medical Sciences. Grant No. 194128. We thank the Water and Electrolyte Research Center staff for their kind cooperation with our research project.
References
- Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16:3365-70.
- [Google Scholar]
- Renal hypoxia and dysoxia after reperfusion of the ischemic kidney. Mol Med. 2008;14:502-16.
- [Google Scholar]
- Renal ischemia/reperfusion injury; from pathophysiology to treatment. J Renal Inj Prev. 2015;4:20-7.
- [Google Scholar]
- The role of renal sympathetic nervous system in the pathogenesis of ischemic acute renal failure. Eur J Pharmacol. 2003;481:241-8.
- [Google Scholar]
- Preconditioning-induced ischemic tolerance: A window into endogenous gearing for cerebroprotection. Exp Transl Stroke Med. 2010;2:2.
- [Google Scholar]
- Ischemic preconditioning ameliorates intestinal injury induced by ischemia-reperfusion in rats. World J Gastroenterol. 2015;21:8081-8.
- [Google Scholar]
- Hypoxic preconditioning protects against ischemic brain injury. NeuroRx. 2004;1:26-35.
- [Google Scholar]
- Hyperoxia-induced preconditioning against renal ischemic injury is mediated by reactive oxygen species but not related to heat shock proteins 70 and 32. Surgery. 2015;157:1014-22.
- [Google Scholar]
- Heat shock preconditioning protects against ER stress-induced apoptosis through the regulation of the BH3-only protein BIM. FEBS Open Bio. 2014;4:813-21.
- [Google Scholar]
- Pharmacological preconditioning with sildenafil: Basic mechanisms and clinical implications. Vascul Pharmacol. 2005;42:219-32.
- [Google Scholar]
- Pharmacological preconditioning with resveratrol: Role of CREB-dependent Bcl-2 signaling via adenosine A3 receptor activation. Am J Physiol Heart Circ Physiol. 2005;288:H328-35.
- [Google Scholar]
- Lipopolysaccharide-induced preconditioning against ischemic injury is associated with changes in toll-like receptor 4 expression in the rat developing brain. Pediatr Res. 2011;70:10-4.
- [Google Scholar]
- Mechanisms of ischemic preconditioning and its application in transplantation. Ann Transplant. 2002;7:12-20.
- [Google Scholar]
- Renal denervation abolishes the protective effects of ischaemic preconditioning on function and haemodynamics in ischaemia-reperfused rat kidneys. Acta Physiol Scand. 2002;174:291-7.
- [Google Scholar]
- Functional and chemical anatomy of the afferent vagal system. Auton Neurosci. 2000;85:1-17.
- [Google Scholar]
- Tension and stretch receptors in gastrointestinal smooth muscle: Re-evaluating vagal mechanoreceptor electrophysiology. Brain Res Brain Res Rev. 2000;34:1-26.
- [Google Scholar]
- Mechanoreceptors of the proximal stomach and perception of gastric distension. Am J Gastroenterol. 2005;100:1704-10.
- [Google Scholar]
- The effect of distension of the stomach on peripheral blood flow in anaesthetized pigs. Exp Physiol. 1996;81:385-96.
- [Google Scholar]
- The primary reflex effects of distension of the stomach on heart rate, arterial pressure and left ventricular contractility in the anaesthetized pig. Pflugers Arch. 1993;425:248-55.
- [Google Scholar]
- The preventive effects of diminazene aceturate in renal ischemia/reperfusion injury in male and female rats. Adv Prev Med. 2014;2014:740647.
- [Google Scholar]
- Sub-diaphragmatic vagal afferent integration of meal-related gastrointestinal signals. Neurosci Biobehav Rev. 1996;20:47-56.
- [Google Scholar]
- Capsaicin-resistant vagal afferent fibers in the rat gastrointestinal tract: Anatomical identification and functional integrity. Brain Res. 1997;746:195-206.
- [Google Scholar]
- Water stimulation of the posterior oral cavity induces inhibition of gastric motility. Am J Physiol Regul Integr Comp Physiol. 2000;279:R778-85.
- [Google Scholar]
- An experimental model for assessment of renal recovery from warm ischemia. Transplantation. 1983;35:198-204.
- [Google Scholar]
- Ischemic preconditioning in the animal kidney, a systematic review and meta-analysis. PLoS One. 2012;7:e32296.
- [Google Scholar]
- VEGF-121 preserves renal microvessel structure and ameliorates secondary renal disease following acute kidney injury. Am J Physiol Renal Physiol. 2008;295:F1648-57.
- [Google Scholar]
- Inflammation is associated with liver function markers, independent of other metabolic risk factors in overweight women. Br J Diabetes Vasc Dis. 2008;8:73-6.
- [Google Scholar]
- Dietary antioxidant and anti-inflammatory intake modifies the effect of cadmium exposure on markers of systemic inflammation and oxidative stress. Environ Res. 2014;131:6-12.
- [Google Scholar]
- Association between plasma alkaline phosphatase and C-reactive protein in Hong Kong Chinese. Clin Chem Lab Med. 2008;46:523-7.
- [Google Scholar]
- Outcome predictability of serum alkaline phosphatase in men with pre-dialysis CKD. Nephrol Dial Transplant. 2010;25:3003-11.
- [Google Scholar]
- Increased serum alkaline phosphatase activity: A possible indicator of renal damage. J Clin Lab Anal. 1991;5:406-9.
- [Google Scholar]
- Causes and consequences of increased sympathetic activity in renal disease. Hypertension. 2004;43:699-706.
- [Google Scholar]
- Stomach distension increases efferent muscle sympathetic nerve activity and blood pressure in healthy humans. J Neurol Sci. 1998;161:148-55.
- [Google Scholar]
- Protective effect of preconditioning on the injury associated to hepatic ischemia-reperfusion in the rat: Role of nitric oxide and adenosine. Hepatology. 1997;25:934-7.
- [Google Scholar]
- Liver ischemic preconditioning is mediated by the inhibitory action of nitric oxide on endothelin. Biochem Biophys Res Commun. 1996;229:264-70.
- [Google Scholar]
- Cardioprotective function of inducible nitric oxide synthase and role of nitric oxide in myocardial ischemia and preconditioning: An overview of a decade of research. J Mol Cell Cardiol. 2001;33:1897-918.
- [Google Scholar]
- Nitric oxide released by gastric mechanoreceptors modulates nicotinic activation of coeliac plexus neurons in the rabbit. Eur J Neurosci. 2000;12:1521-4.
- [Google Scholar]
- Contribution of nitric oxide to the protective effects of ischemic preconditioning in ischemia-reperfused rat kidneys. J Lab Clin Med. 2001;138:50-8.
- [Google Scholar]




