

Translate this page into:
Cholemic Nephrosis from Acute Hepatitis E Virus Infection: A Forgotten Entity?
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Cholemic nephrosis (also known as bile cast nephropathy) is an underreported cause of acute kidney injury (AKI) and is usually seen in patients with sustained cholestasis, such as those with advanced cirrhosis or acute on chronic liver failure (ACLF). Hepatitis E virus (HEV) infection, a common cause of acute infectious hepatitis with acute cholestasis, has been associated with renal manifestations such as acute tubular necrosis (ATN) and glomerulonephritis, but the current literature is scant on acute HEV infection causing cholemic nephrosis with AKI.
A 50-year-old male was admitted with a 2-week history of acute febrile illness and 1-week onset of progressive jaundice. He had good urine output. He denied any alcohol intake, history of blood transfusions, sick contacts, or performing any high-risk sexual activity. Upon examination, his temperature was 39°C, blood pressure was 160/90 mmHg, and the heart rate was 110. He had significant icterus. His urine output was more than 1 L/day.
His laboratory investigations revealed hemoglobin of 8.9 g/dl and normal white blood cell (WBC) and platelet count. His total bilirubin was 33.9 mg/dl with a predominant direct component of 20 mg/dl. His alanine aminotransferase, aspartate aminotransferase, and alkaline phosphatase were 157, 131, and 692 IU/L, respectively. His coagulation profile was normal. His kidney function was grossly deranged with a urea and creatinine level of 197 mg/dl and 5.6 mg/dl, respectively. His serum sodium (Na) was 128 mEq/L and potassium (K) was 2.8 mEq/L. His urine sediment was bland with no proteinuria and no red blood cells and WBCs. Urinary spot Na was 35 mEq/L.
Patient's peripheral blood smear did not reveal any parasites. Blood culture and antigen testing for malaria were negative. An IgM antibody test for HEV was positive. Serologic tests for hepatitis A, B, and C were negative. He was managed conservatively along the lines of prerenal AKI with intravenous (IV) fluids, IV albumin, and K repletion. Ultrasound-guided renal biopsy was performed which revealed normal appearing glomeruli with evidence of diffuse acute tubular injury, and over 50% of all tubules had intraluminal bile casts, which was confirmed with Fouchet's stain [Figure 1]. A diagnosis of cholemic nephrosis causing nonoliguric AKI, likely resulting from acute HEV infection, was made. With conservative treatment, the patient made complete recovery of liver and renal function with both normalizing within 4 weeks. His serum creatinine and total bilirubin at 6-week follow-up were 1.2 and 0.3 mg/dl, respectively, and continued to be stable.
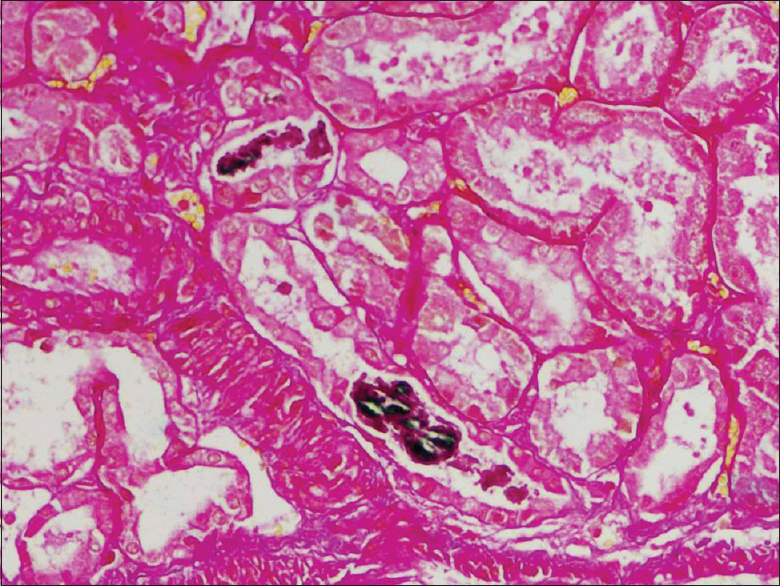
- Tubular bile casts (Fouchet's stain)
Cholemic nephrosis (bile cast nephropathy), although underreported, has been shown to be the underlying pathology associated with AKI in majority of patients with cholestasis from decompensated cirrhosis and ACLF.[1] Conventionally, the diagnosis is made with the coexistence of diffuse tubular injury along with tubular intraluminal bile casts. The pathogenesis has not been fully elucidated yet, but direct tubular toxicity from bilirubin and bile salts and tubular intraluminal obstruction (such as which happens in myeloma kidney) are the two proposed mechanisms.[2] In general, this involves distal tubules but sometimes affects the proximal collecting tubules as well.[3]
HEV infection most often causes a self-limited acute hepatitis and is the most common cause of acute infectious hepatitis in the developing countries. HEV infection has been shown to be associated with renal manifestations[4] such as ATN and various glomerulonephritides such as IgA nephropathy and membranoproliferative glomerulonephritis.[5] Our patient had biopsy-proven cholemic nephrosis as evidenced by diffuse acute tubular injury associated with extensive intraluminal bile casts. His kidney function gradually recovered with the resolution of hyperbilirubinemia with conservative management.
Cholestasis from acute HEV infection may be associated with cholemic nephrosis and AKI.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Bile cast nephropathy in patients with acute kidney injury due to hepatorenal syndrome: A Postmortem kidney biopsy study. J Clin Transl Hepatol. 2017;5:92-100.
- [Google Scholar]
- The pathology of jaundice-related renal insufficiency: Cholemic nephrosis revisited. J Nephrol. 2006;19:229-33.
- [Google Scholar]
- A73-year-old male with jaundice and acute kidney injury. Bile cast nephropathy. Neth J Med. 2014;72:95-99.
- [Google Scholar]
- Extra-hepatic manifestations associated with hepatitis E virus infection: A comprehensive review of the literature. Gastroenterol Rep (Oxf). 2016;4:1-5.
- [Google Scholar]
- Hepatitis E virus and the kidney in solid-organ transplant patients. Transplantation. 2012;93:617-23.
- [Google Scholar]




