

Translate this page into:
Persistent Left Superior Vena Cava in a Hemodialysis Patient
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Awareness of persistent left superior vena cava (PLSVC), a rare congenital variant is helpful to a clinician to avoid the unnecessary complications. We report a case of PLSVC in a patient with chronic kidney disease which was identified following a difficult catheterization into the right internal jugular vein (IJV). The catheterization was attempted through the left IJV and the position of which could not be confirmed with check radiograph and two-dimensional echo. PLSVC was suspected in the computed tomography angiography and was confirmed following digital subtraction angiography.
Keywords
Catheterization
hemodialysis
persistent left superior vena cava

Introduction
Internal jugular vein (IJV) is most commonly used temporary vascular access for hemodialysis. Awareness of anatomical variations of the vessels in the cervical and thorax region is necessary to prevent the avoidable complications. Persistent left superior vena cava (PLSVC) is the most common congenital thoracic venous anomaly found in 0.3%–0.5% of the general population and 4% of the patients with congenital heart disease.[1234567] We report a case of PLSVC, which was accidentally detected after a jugular catheterization procedure.
Case Report
A 35-year-old male hypertensive patient presented to emergency room with accelerated hypertension and pulmonary edema. He was diagnosed as chronic kidney disease (CKD) 2 years before this admission with a base line serum creatinine of 3.2 mg/dl and was under follow up elsewhere. On admission, the patient was pale and had bilateral pedal edema. His blood pressure was 200/120 mmHg. On auscultation, bilateral basal crepitations were heard. Routine blood investigations revealed the following findings: Hemoglobin: 8.6 mg/dl, serum creatinine: 10 mg/dl, blood urea: 162 mg/dl, sodium: 136 mg/dl, potassium: 4.6 mg/dl, parathyroid hormone: 332 pg/ml, total cholesterol: 231 mg/dl high-density lipoprotein: 34 mg/dl, low-density lipoprotein: 76 mg/dl. Ultrasound kidney, ureter, bladder showed bilateral small kidneys. He was diagnosed as CKD Stage V (estimated glomerular filtration rate 6 ml/min/1.73 m2 [CKD-EPI]) and renal replacement therapy was planned for the patient. A double-lumen noncuffed dialysis catheter was attempted on the right IJV, but the needle could not be negotiated down into the IJV. The subsequent neck vessel Doppler revealed a thrombus in the right IJV, and then, the procedure was planned through the left IJV.
The dialysis catheter was placed in the left IJV and the flow patency was checked. A check radiograph showed abnormal position of catheter tip, along the left mediastinal border [Figure 1]. The blood gas analysis confirmed the venous blood (pH 7.29; PCO2, 58 mmHg; PO2, 38 mm Hg). The tip of the dialysis catheter could not be identified appropriately with the two-dimensional echo as well. We further went ahead with the computed tomography angiography, which revealed a doubtful PLSVC. Digital subtraction angiography was done subsequently and the PLSVC joining the right atrium was appreciated [Figure 2]. Hemodialysis was initiated through the left IJV.
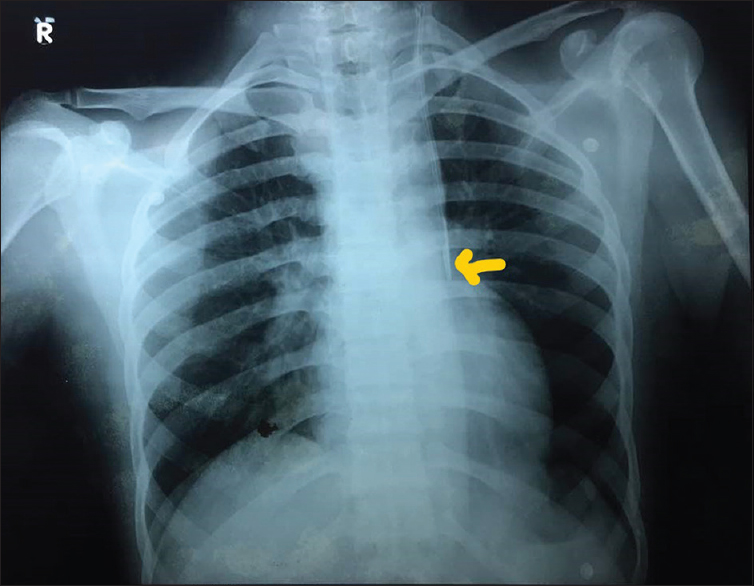
- Dialysis catheter tip at the left mediastinal border (yellow arrow)
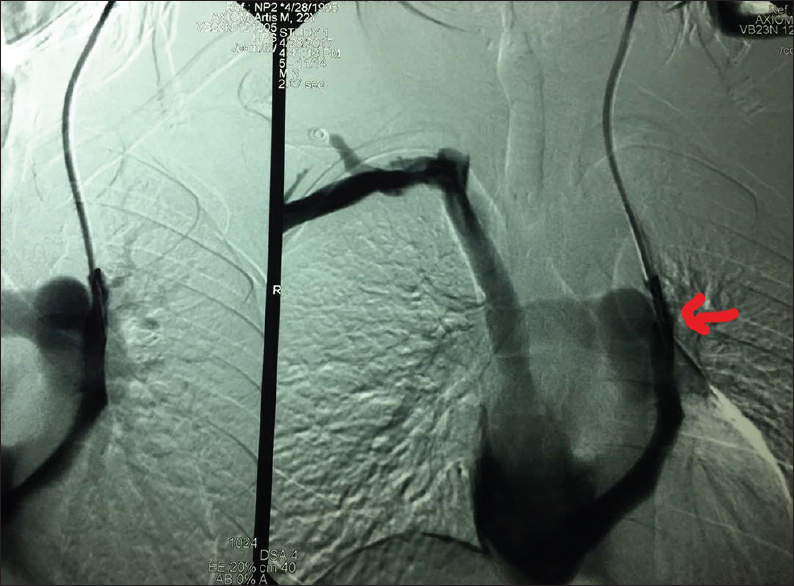
- Digital subtraction angiography showing the persistent left superior vena cava (red arrow)
Discussion
Castellanos first demonstrated the left superior vena cava (LSVC) by angiocardiography.[8] The incidence of LSVC varied from 0.3% in healthy individuals to 4.3% in patients with congenital heart disease. Hairston stated that the PLSVC is the most common variant of abnormal systemic venous entry into the heart.
John Marshall gave the first embryological explanation for PLSVC in 1850.[9] During the 8th week of gestation, an anastomosis forms between right and left superior cardinal veins resulting in the innominate (or brachiocephalic) vein. The cephalic portion of superior cardinal veins form the IJVs. The caudal portion of the right superior vein forms the normal right-sided superior vena cava, while the portion of the left superior cardinal vein caudal to the innominate vein normally regresses to become “ligament of Marshall.” If this normal regression of the left superior cardinal vein fails to occur, a persistent left-sided vascular structure that empties into the coronary sinus, results into PLSVC.
Schummer et al.[10] suggested a classification system of superior vena cava according to the positioning of a central venous catheter on the chest radiograph: Type I, normal anatomy; Type II, only PLSVC; Type IIIa, right and left superior vena cava with connection; and Type IIIb, right and left superior vena cava without connection.
Our patient was found to have a Type IIIb superior vena cava. Placement of a catheter into a PLSVC can be mistaken for placement into subclavian or carotid artery, descending aorta, internal thoracic vein, superior intercostal vein, pericardiophrenic vein, mediastinum, pericardium, or pleural space. Furthermore, cardiac arrhythmias including ventricular fibrillation and atrial septal defects have been associated with PLSVC.[11] 92% of PLSVC drain into the coronary sinus and thence into the right atrium. In this circumstance, the coronary sinus is usually large due to increased blood flow through it. The rest of 8% drain into the left atrium creating right to left shunt. This variant is potentially dangerous as the cannula in PLSVC may give rise to systemic embolization of air or thrombus.
The clinicians should be aware of this anatomic variant to prevent the complications and the unnecessary dilemma regarding the appropriate position of the catheters in place.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Persistent left superior vena cava. Radiologic and clinical significance. Radiology. 1972;103:375-81.
- [Google Scholar]
- Discovery of left-sided superior vena cava during central venous catheterization. Br J Anaesth. 1998;81:260-1.
- [Google Scholar]
- Left-sided superior vena cava: A not-so-unusual vascular anomaly discovered during central venous and pulmonary artery catheterization. Crit Care Med. 1992;20:1119-22.
- [Google Scholar]
- Persistent left superior vena cava; survey of world literature and report of thirty additional cases. Angiology. 1954;5:90-132.
- [Google Scholar]
- On the development of great anterior veins in man and mammalian: Including an account of certain remnants of fetal structure found in the adult, a comparative view of these great veins in the different mammalia and an analysis of their occasional peculiarities in the human subject. Philos Trans R Soc Lond. 1850;40:133-50.
- [Google Scholar]
- Persistent left superior vena cava and central venous catheter position: Clinical impact illustrated by four cases. Surg Radiol Anat. 2003;25:315-21.
- [Google Scholar]
- Unusual placement of a dialysis catheter: Persistent left superior vena cava. Am J Kidney Dis. 2004;43:365-7.
- [Google Scholar]




