

Translate this page into:
Healthcare in India and Violence against Doctors: The Missing links
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Death is the destination we all share, no one has ever escaped it. And that is as it should be, because death is very likely the single best invention of life.
…………… Steve Jobs
With the limitations of medical science, even in 21st century, it is impossible to save every patient even in the best of the hospitals in the world, and in India, a majority of the hospitals are far from being best in the world. Therefore, correlating any death of the patient with negligence of the doctor and violently reacting against him is not an expected human behavior, as aptly written[1]“It can only be termed animal behavior when anyone attacks doctors.”
In the healthcare history, for the first time on 12th September 1978, elected representatives from 134 countries and 67 international organizations unanimously accepted “Alma-Ata Declaration” (of united nation),… “expressing the need for urgent action by all government, all health and development workers, and the world community to protect and promote the health of all the people of the world.”[2] The Declaration had two core principles in it:
Health was indeed a human right and,
In order to maintain the same, several social and economic sectors, in addition to health sector, needed to be actively involved and show results.
However, even after 40 years, we still are dreaming for “health for all.”
Being in medical profession as a healthcare provider for the past 40 years, as trainee, junior faculty, senior faculty, and lately heading a busy clinical department and also being a patient in the past and attendant for the admitted parents, I thought of writing about healthcare status of the country in the background of published information.
Healthcare Financing
With a population of over 1.32 billion, India is well on its way to upstage China as the world's largest country. Our population is on one hand our greatest strength and on the other greatest weakness. By 2020, the age of an average Indian will be about 29 years. While a young India is great for the industry and economy, the great Indian middle class is teetering on the brink of a major crisis – a healthcare crisis, one of the reasons being poor public funding. Healthcare system in any country is based on public and private system. India's public healthcare system is a near disaster primarily due to the low funding. In fact, among the newly industrialized nations and even among the BRICS countries, India's per capita spending on healthcare is dismal. If we see the public funding as the percentage of gross domestic product (GDP), for the past 15 years, it has remained very low near 1.2%[3] [Figure 1], nearly 20% of overall health expenditure in the country, with 80% being provided by private sector [Figure 2]. Even in 2019–20 financial year, it has been only increased to 1.29% of GDP.
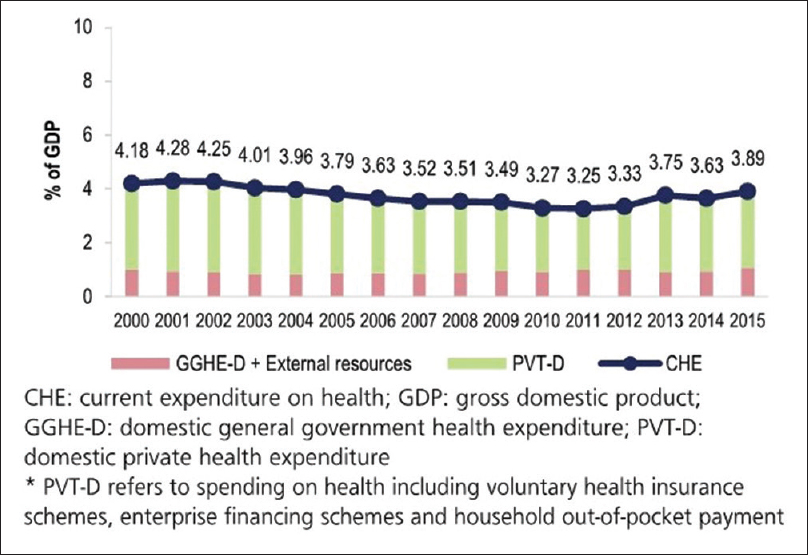
- Government and private expenditure on health as a % of GDP 2000-2015

- Public and private healthcare. Private healthcare in India cost about four times more than public sector yet majority of all cases are treated by the private sector
In principle, government health services are available to all citizens under the tax-financed public system. In practice, bottlenecks in accessing such services compel households to seek private care, resulting in high out-of-pocket payments (69% of total expenditure).
Infrastructure
Healthcare is expected to be the right of every individual.[4] About 60% (700 million) of the population of India is rural population, and to cater their health needs, there are 156,231 subcenters, 25,650 primary health centers, and 5624 community health centers in India as on 31st March 2017 [Table 1]. There are 23,582 hospitals having 710,761 beds in the country, 19,810 hospitals are in the rural area with 279,588 beds, and 3772 hospitals are in the urban area with 431,173 beds. The country has 476 medical colleges, 313 dental colleges for Bachelor of Dental Surgery, and 249 dental colleges for Master of Dental Surgery.
| Infrastructure | Number | One unit for number of populations |
|---|---|---|
| Hospitals | 23,582 | 54,028 |
| Hospitals in urban area | 3772 | 135,110 |
| Hospital in rural area | 19,810 | 38,589 |
| Number of beds | 710,761 | 1792 |
| Number of bed in urban area | 431,173 | 1181 |
| Number of beds in rural area | 279,588 | 2734 |
| Subcenter in rural area | 156,231 | 5000 |
| Primary health centre | 25,650 | 30,000 |
| Community health center | 5624 | 150,000 |
There are no global norms about the number of hospitals or number of beds for the number of populations. A report by World Health Organization (WHO) about the number of beds in South East Asia (SEA) region and the world average shows that between 2005 and 2012, the average number of beds in India was 9 beds per 10,000 population, while the world average was 30 per 10,000 population. Even SEA region also had an average of 11 beds per 10,000 population [Figure 3].[5]

- Provision of hospital beds and other facilities in SEAR countries, 2005-2012
Manpower
In addition to infrastructure, human resources for health are equally, rather more important component of public health delivery. Availability of adequate number of human resources with appropriate expertise and their suitable deployment at different levels of healthcare setup are essential for providing effective healthcare services for the population. Table 2 shows current manpower related to health sector.
| Manpower designation | Number | One per number of populations | WHO norms |
|---|---|---|---|
| Allopathic doctor | 988,922 | 1668** | 1000[7] |
| Dental surgeon | 7239 | 176,004 | 7500[8] |
| AYUSH care providers | 773,668 | 1646 | No defined norm |
| Ayurvedic doctor | 428,884 | 2970 | No defined norm |
| Unani doctor | 49,566 | 25,705 | No defined norm |
| Siddha doctor | 8505 | 14,905 | No defined norm |
| Naturopathic doctor | 2242 | 568,285 | No defined norm |
| Homeopathic doctor | 284,471 | 4478 | No defined norm |
| ALL nursing personals | 2,878,182 | 442 | 250[9] |
| ANM | 841,279 | 1514 | No defined norm |
| Registered nurse | 1,980,536 | 643 | No defined norm |
| Lady health visitor | 56,367 | 22,603 | No defined norm |
| Pharmacist | 907,132 | 1404 | No defined norm |
WHO: World Health Organization. Source: National health profile India, 2018. **Source: Medical Council of India
What can be said about the comparison of India with Western world, even comparison to SEA region is also not very encouraging. A recent WHO report suggests that India is almost comparable to other countries of the region and even below than Maldives [Figure 4]. While 44.6 global health workforce was suggested in 2016 for 10,000 population, India had nearly 29 per 10,000 population.

- Aggregate density of physician, nurses and midwives per 10,000 population in SEAR countries
Furthermore, in addition to comparison to other SEA countries, what is more important is that India should have progressed in terms of manpower with time. However, if we see the change in health workforce between 2008 and 2016, not only it has remained much below global recommendation but also there had been very marginal change in midwifery and hardly any change in doctors [Figure 5].

- Decade for health workforce in the South east Asia Region 2015-2024 Second review of progress, 2018
The crisis in India's public health infrastructure is laid bare by recent official statistics that reveal that the country faces a shortfall of around 82% in specialists like surgeons, gynecologists, physicians, and pediatrician; almost 40% in laboratory technicians; and a critical 12%–16% shortage of nurses and pharmacists at community and primary health centers[10] [Figure 6]. In most states, the gap between required and available specialist in these centers, which are often the first port of call and are also expected to act as early warning and referral system, is in the range of 80%–90%.

- Deficit of specialist at community health centres
Doctors are being criticized that very few wish to go to primary care center. However, one should also see their point of view. Doctors also need adequate facilities at the health centers to provide medical care. In addition, a doctor has his own family and children to support, needs good education systems for children's education, and needs a reasonably good quality of life. Often, we compare our primary health centers with western setup. Western setups not only have adequate infrastructure but also have reasonably good quality of life at places where primary healthcare is being provided.
Patient Attendants in the Hospital
Currently, there is a mix picture as far as the number of attendants of patient in the hospitals is concerned. In many nuclear urban families, there are very few relations and they are also not free to come as attendant with patient; while in some families, there are too many attendants with the patient. In India, in a majority of public hospitals, though the numbers of attendants are restricted as a policy, attendants have become a necessity. Attendants are required not only for arranging medicines in emergency as well as on routine basis but also for various patient-related work ranging from biological sample delivery to laboratory, collection of reports, shifting of patients for various tests, pulling the trolley having patient, providing bed pan, watching the IV fluid administration, Ryle's tube feeding, providing exercise to patient, and so on. To some degree, it is not only due to shortage of healthcare personals in public hospital but also because of indifferent and casual attitude of staff in taking care of patients.
If all the above is required from patient's attendants, how can we restrict the number of attendants with a patient? Even the patient outcome is also good if one has alert committed attendant with him or her. In most public hospitals, attendants also get exhausted if a patient is admitted for few days. While the patient himself may not be able to visualize care being provided, it is the attendants who are mostly aware of what is being done for their patients. It is one of the reasons that people who can afford wish to go to a private setup not for the patient but for attendant's comfort also, may be at the expense of some other compromises. No surprise that in such a situation if a patient dies, there is violent reaction by the attendants.
Another related issue, which has worsened this situation, is a general policy that public hospitals nowadays do not employ regular class III–IV employees and all such facilities are outsourced. These outsourced staff has no commitment to hospital and patients and while one day the same person works as hospital attendant, the next day he or she may be working as sanitary attendant, causing confusion in the mind of educated patients about the level of proficiency these staff have.
In private setup, there is reasonably good quality security restricting the entry of attendants in the hospital, while in government setup, the quality of security is such that sometimes security person needs his own security from miscreants. I am told that often these security persons do not get their wages as promised by the security agency/contractor. Also, they hardly have any gadget, which can be used at the time of need from the security point of view. One can guess how effective they will be.
Machinery, Consumables, and Medicines
In addition to infrastructure and manpower, the third important requirements in any healthcare setting are machines and consumables including medicines. In many public hospitals, medicines and consumables are not available in required quantity and some are not available at all. In such situations, asking patients' relatives to purchase consumables at the time of emergency makes it very difficult for the relatives, particularly when it is odd time and when only a lady attendant is there. Nuclear families being the norm nowadays, such situations are becoming very common.
Even many big public hospitals in the country do not have round-the-clock dispensary from where relatives can buy the medicines and consumables at odd hours. The treating doctor is helpless in such situations and neither he can nor he is supposed to arrange such things. These are to be provided by the “system.” A doctor can only use his professional competence to treat patients with the facilities available. Once such effective “system” is not in place, and there is deficiency in management of patient due to need of appropriate medicine or consumable, relatives react to the doctors, who are in front of relatives at that point of time. People who are expected to make such “system” in place, like medical superintendent, director, and administrative officers, will not be there in front of the patients to bear the brunt. “Poor doctor” has to face all the consequences. Has anybody read in media that medical superintendent, or director, or nurse, or hospital attendant was beaten by relatives? It is always the doctor.
The purchasing system in public hospital also has an issue. When it comes to funds, people are hesitant to take decision/responsibility. The result is that the same file for purchasing moves from one direction from lower level to upper level and back, and if there is any query, the same route is followed again and again. This results in purchasing taking too much of the time. Other than time, another issue in purchasing is the policy that L-1 (lowest prize bid item) is to be purchased, whether the item is of standard or not and whether post sale service is expected to be satisfactory or not. All public healthcare systems are bound to purchase L-1. Once this L-1 machine or consumables do not function properly, not only patient care is affected but also doctor is blamed for nonfunctioning machine or poor-quality consumables. Another issue which has recently come into effect is the issue of “Make in India.” There is general direction to encourage purchasing of “Make in India” products. Not that Indian manufacturers are not competent but their competence and product quality have to be proven first before asking to prioritize for “Make in India.”
Emergency Care in Hospital
It is terms like “The Golden Hour” and the “Platinum Ten Minutes” that typify the importance of Emergency Medical Services (EMS) all over the world. It is a well-accepted fact that a patient who receives initial care from well-trained professionals within 15–20 min of an emergency has the greatest chance of survival. EMS is one of the most essential parts of the overall healthcare system as it saves lives by providing care immediately. However, the state of EMS varies drastically among different hospitals in India. In spite of the development in the healthcare sector over the past decades, India is yet to create a single, comprehensive EMS that can be accessed throughout the country. When compared to developed countries with proper emergency systems in place, there is no single system which could play a major role in managing emergency medical services in India. There is a fragmented system in place to attend the emergencies in the country.
In most of the public hospitals in India, it is often the junior most medical personal (junior resident or house officer) who is the first contact person with the patient and anxious attendant in emergency. Not only that this doctor may not be most efficient to handle emergency but also much more important is that he or she often lacks communication skills. The result is that if by chance a patient could not be saved, there is outburst of anger against the doctors, and experiences suggest that often emergency is the most common place of assault on doctors.
In most public hospitals in India, emergency beds are limited. Hospitals are often forced to make trolley as a regular bed and decrease the basic necessity of space requirement between two beds, thus increasing the risk of cross-infection. Figure 7 depicts one such situation, where trolleys work as beds alongside regular beds. Doctors even find it difficult to move in between the beds to take care of the patients [Figure 8]. One can imagine the scenario, if a patient collapses and there is need of resuscitation, what will be the situation in such circumstances.

- Usual scene in a public hospital in India

- Common situation in an emergency area of a public hospital
In addition, other usual issues in most public hospital emergency areas are limited number of wheel chairs and trolleys, absence or paucity of hospital attendants to shift the patient, long queues, delay in screening the patient to shift to appropriate triage area, and so on. It will not be rare to see some patients carry their own wheel chairs, if they have to visit healthcare facility frequently.
There is a fragmented system in place for emergencies in the country. 102 is the emergency telephone number for ambulance in many parts of India. There are different emergency numbers in India's 29 states and seven Union Territories. Hospitals in the country provide different telephone numbers for ambulance services. Clearly, India is in need of proper accessible emergency medical services. The existing fragmented system also falls terribly short of meeting the demand.
Issue of Generic Medicine
There is no doubt that availability of quality affordable medicines is a key component of a successful healthcare system in any country. Considering this, the concept of “generic” medicine evolved. However, before all public sector hospitals adopt “generic medicine,” the quality of “generic medicine” must be ensured. Also, one should understand what is “generic” medicine. It is only the innovator whose medicines are labeled “branded” medicine. Any medicine other than that of the innovator is basically “generic” medicine. Other than the innovators, pharmaceuticals which give a name to a compound is often called “branded generic.” Actual “generic” is basically sold with the pharmacological name of the drug along with its manufacturer's name. All generic medicines are cheaper than branded medicines because companies that produce such medicine do not spend time and money on research, which is also the main reason why the branded medicines are expensive. Despite the low price, generic medicines should be as effective as branded medicines since they use the same active ingredients.
Indian generics are particularly cheap among generic drugs because India is a cost-competitive site for pharmaceutical manufacturers. A recent report shows[11] that facilities producing active pharmaceutical ingredient (API), a vital functional component in a drug in India, are four times more than those in the United States. The reason behind is that production of APIs involves dangerous chemicals, and India has a looser environmental and labor policies, so companies prefer sites in India to avoid higher cost. Considering the lower production cost, it is not unexpected that Indian generic medicines are cheaper. If Karan Thapar is to be believed, I quote “Often generic drugs manufacturers in India produce medicines of higher quality for European and American markets, where regulation is tighter, whilst blithely selling inferior and ineffective drugs in India. You and I may keep taking generic drugs believing they're efficacious, but we're being made fools of. And the authorities simply don't care”.[12]
Branded generic are actually also generic and their prices are required to be controlled. Branded generic may be needed to be included into the list of essential medicines. If that is a difficult issue, then there is a need of restricting the number of generic medicines for one pharmaceutical compound and the quality of these generic medicines needs to be authenticated, regulated, and ensured. Otherwise, professionals and public will not have faith on generic medicines. In many public hospitals, generic medicines, which are available, are often not found to be effective, and if the same patient purchases branded generic, it does make a difference in response to therapy.
The Medical Council of India code of ethics prescribes that doctors in India should write prescription with generic medicines; but with a large number of generic medicines available for one pharmaceutical, it will be upto the chemist to decide which generic will be given to patients. There is probably a need to regulate the number of generic for one product and ensure its quality and availability to common man at affordable prize.
Public Versus Private Sector
Experts say that a large number of deaths in India occur due to lack of medical treatment and facilities. The percentage of death rate in India per 1000 people is 7.3% as of 2015,[13] which continues to increase every year because of the lack of quality medical care and soaring cost of treatments. We are facing a major healthcare crisis. Healthcare crisis calls for basic healthcare needs such as medical care, proper medical professionals and aid, and availability of quality hospitals and healthcare systems; a criterion which urges the mass to choose between public and private healthcare services in India.
Public healthcare systems get their funds from the government, which makes it mandatory for them to cater to everyone. Hence, they are in no position to turn anyone away even if patients are penniless. As a result, citizens are forced to stand in long waiting lines; many of them ultimately end up going to private hospitals for timely treatment and often become below poverty line due to exuberant out-of-pocket expenses.
Let us compare some of the facilities between public and private hospitals, which are actually necessities for a patient and family in a healthcare setting.
Overcrowding: The fact that public hospitals are governed by the government and the cost of available treatment is less is the sole reason that a huge population of India, who cannot bear the cost of private setup, are forced to come to these public hospitals. The public hospitals, which have excelled in term of quality of care, bear the maximum brunt. They are affected by their own quality. The common scene in most public hospitals in outpatients [Figure 9] and in patients [Figure 10] is known to Indian public and healthcare providers. In outdoor, patients do not have adequate sitting arrangement and most public hospitals do not have air conditioning in these crowded places. In such situation, standing for hours is difficult for a healthy person, what to say for a sick patient and their attendant.

- Common scene in an outpatient in many public hospital

- Common scene in in-patient hospital in many public hospitals
One can imagine that in such scenario, any lack of communication or delay in management is likely to cause outburst of attendant toward medical personals, the easiest target being doctor.
Such situations are not seen in private setup, where there are a fewer number of patients, there are facilities of sitting arrangement in usually air condition environment, patients come at their appointment time, waiting time is less, and hence they meet the doctor and return home soon. But obviously at high cost, which most cannot afford in India.
Water: Every human being needs water for survival. Most of the public healthcare facilities do not have facilities of safe and clean drinking water in all the areas of the hospital. Even in so-called reputed public hospital in the capital city of Delhi, there is no regular water facility for drinking water in outpatients where doctors, patients, and attendants have to remain for long hours.
Food: Not only patients but also their attendants need food. Time has gone when patients' attendants were bringing food from home for the patient. Today's reality is that in most situations, both patients and their attendants take food from the hospital. In most public hospital, there is limited facility of palatable food at reasonable cost, and almost in all, this facility is not there round the clock. Sick patients with attendant in the absence of palatable food makes them potential litigant against healthcare providers. Again, brunt is on doctors rather than administration, who is supposed to provide such basic facilities. In private hospital, a good round-the-clock canteen, often from a food chain provider, is usually available as these facilities are also source of income to the hospital. Whatsoever, at least affordable patients do get the food.
Waiting area: It is easy to ask patient's attendants to go away from the ward to avoid cross-infection and for smooth management of ward. But think from their perspective. Where should they go? In almost all public hospitals, there is no organized waiting area for attendants. In many hospitals, they wait on footpath or by the side of the roads. Furthermore, they are also needed for various activities to the system in public hospitals, so they cannot disappear. As against this, in private hospital, in addition to proper sitting arrangement in waiting area, often the area has announcement system to call attendants at the time of need, and also, most of these areas have television for attendant entertainment also.
Cleanliness: Swachh Bharat Abhiyan of Hon. Prime Minister definitely has made a change in hospitals also. But still in most public hospital cleanliness is not a priority. There is lack of concept both in hospital staff and attendants that it is necessary to prevent a hospital-acquired infection, which is an important cause of morbidity and mortality. In private setup, this is necessary for keeping image of the hospital and to satisfy the type of people coming to such hospitals. Another important difference with regard to cleaning the hospital is that in public hospital cleaning is often done at the busy morning time when doctors are taking round of the ward, while in private setup, it is done in the night or early morning when there is minimal disturbance to patients and attendants and hospital working.
It will be tragic if we start comparing toilet and washrooms between public hospitals and private setup. Not only the numbers are very limited but also the condition of washrooms is in pathetic shape that a large number of patients and staff avoid using them. An additional issue is that there is hardly a separate washroom in public hospitals for doctors and other medical staff even in the so-called reputed public hospitals in NCR region, what to say for smaller cities.
Parking: In the absence of good public transport system in most of the cities in India, a large number of people travel by their own vehicle. However, for public hospital, this situation is changing dramatically. There are very limited facilities of parking the vehicles and some time if it is available, it is far away from main hospital building. The results are that even people who have vehicle nowadays prefer to come to hospital by taxis or public transport system. If the patient is alone, then it is mostly impossible to come and park his vehicle and able to show to the doctor. In some of the organized big public hospital, a transport system is available to take the patients from parking lot to other places within hospital premises. But this is an exception rather than common. In private hospital, parking is given importance and it also becomes some source of additional income to hospital. To the extent, some private hospitals do have valet parking system also. Types of people who attend private hospitals do not mind paying little extra for such organized system.
Payment system: Private hospitals mostly have one-window payment system; a sizeable component of cost involved for healthcare is taken in advance also. A majority of credit cards are accepted, making payment system user-friendly. In public hospital, often there are different windows for payment for different purposes. So, if four investigations are to be done, no surprise if the patient has to pay at four places. Credit card payment system is mostly not available, nor the type of patients who come to these hospitals have credit cards.
Consumables: In most public hospitals, all consumables and medicines are not available and it is not uncommon that relations are asked to buy these items from open market, often in odd hours making it very cumbersome for the attendant. In private hospitals, relations do not need to bother for purchasing consumables and just pay at the time of discharge. However, this comes at a very high cost. Private setup often forces patients to take consumables from the shops within premises of hospitals, which is at high cost. Most private hospitals purchase in bulk at much lower cost and sell them at maximum retail price, gaining huge margins on consumables and medicines.
Education status of patient: Patients attending public hospital are not only often poor but also their education standard is usually lower than those attending private hospital, though the generalization may not be true. A detail explanation of disease, potential treatment, and outcome is difficult to explain to them. Actual informed consent is difficult to obtain. After a time, the final word ”doctor you do what you think is best for me” is the usual attitude. Taking part in decision process related to treatment by the patients and attendants in government-run hospital is very unusual. Though they will not shy for blaming if things go wrong with one approach of treatment and often become violent also blaming treating doctors. Patients who are little affordable and educated, mostly go to private setup or come to public set-up with the so-called through some very important person (VIP) or with personal contacts.
Targets in private setup: Many private hospitals setup targets for an employed doctor. “Target” means that a doctor has to generate “X” amount of money to compensate for his own emoluments/salary. I am told by colleagues in private setup that for any emoluments, one has to generate approximately 10 times of the emolument. A usual emolument for a nephrologist on fixed salary in private setup varies from $ 70,000 to $400,000 per year, later for very few of them. One can imagine that a retired 60-year-old professor from an academic institution now working in private setup is questioned by a 25-year-old MBA, questioning him for incomplete target. A doctor who is getting say $70,000 per year has to generate $700,000 per year for the hospital to continue getting that much. This often forces some doctors in private setup to do things, the so-called unethical practice, doing investigation, procedures, and surgeries, which are not actually required just to complete his target or else he has to quit the hospital. I must point out that this may not be prevalent in all private hospitals and with all doctors. Everybody is not the same, but a many do this.
New-Generation Residents
Today's resident is much wiser and more practical than before. For them every work in the hospital is a ladder on which they wish to go up and use that for their future life. Many of them are very clear about what they wish to do in future so they are more interested to work in those areas in the hospital which will help them in their future venture. Often, they lack communication skill, and lack of communication, no communication, or the way they communicate with the patients and their attendants, particularly when the patient is sick, often becomes the reason of altercation with the attendants. There is nothing in the medical curriculum about the communication skill, which mostly comes with experience, and as that experience is lacking in many residents, they become the most common target for argument with the patient's relatives. I have no intention to question the competency of resident in care of patients, but in healthcare setup, one needs not only science of medicine but also art.
In view of long years of study before settling in life when compared to other streams, all India competition at every stage of career making it uncertain to get the next stage, reservation at every stage, and more-super specialization rather than family physician setup, it is not a surprise that many bright students are not opting medical profession in the country. With repeated violent behavior against doctor, it is not a surprise that younger generation is hesitant to take medical stream [Figure 11].

- Cartoon for feelings against joining medical profession
In spite of so many hurdles, still the number of applicants for medical entrance examination in India has increased significantly in the past few years [Figure 12]. Still it is considered a noble profession and expected to command a reasonable respect, which may get eroded if such frequent violent behavior continues against doctors by the public/relations of the patients. Furthermore, this respect has already been eroded due to the profession being taken under consumer protection act and demand and supply gap in infrastructure and human resource in healthcare sector.

- Number of applicants for medical entrance examination in India
Other Healthcare Workers
Healthcare facility is a place where providing healthcare to patient is the combined effort of the teams involving doctors, nursing officer, hospital and sanitary attendants, laboratory persons under administrative supervision of policy makers like medical superintendent, head of the hospital, and administrator. However, whether it is emergency, regular inpatient ward, outpatient area, or procedure room, if there is any complication, fault, or mismanagement because of any team member, it is the doctor only who comes under attack by the patient's attendant. Has any one of us seen the report that medical superintendent or director or nurse or hospital attendants are attacked by the relatives? The answer is big NO.
However, none of the team member mentioned above is under doctor administratively, and whenever any complaint against nonperformance of any other team member is made by the doctors, their union and administrative issue comes in between for taking any action against the nonperformer. Policy makers in the public system are often heard saying that “nothing can be done against them because of their union.” So, basically doctors have to work with and depend on other paramedical staff, which is not under their control, and on top of that doctors are also blamed for their faults.
Issues at the Level of Policy Making
For India, one of the major drawbacks has been that health has never remained a priority for successive government since independence, without realizing that “healthy nation is a wealthy nation.” Public actors in the Indian healthcare system include the Ministry of Health and Family Welfare (MOHFW), state governments, and municipal and local bodies. Each state has its own Directorate of Health Services (DHS) and Department of Health and Family Welfare. District-level health services provide a link between each state and primary care services.
Other agencies involved in health system governance include the Insurance Regulatory and Development Authority, which regulates the health insurance industry, and the National eHealth Authority, which is to become the authority for development of an integrated health information system.[14] There is lack of clarity in India with respect to which entities are responsible for regulating the private sector and for ensuring quality of care, as there are multiple agencies under different ministries.
Can India Have Universal Health Coverage (UHC)?
In India, the National Health Protection Scheme or “Modicare” was initiated under the Union Budget 2018.[15] The scheme aims to provide health insurance to 100 million families (500 million individual), with a cover of Rs. 5 lakh each. Though India seems to be making progress in terms of its move toward UHC, which it plans to attain in 2030, there are certain healthcare issues that need to be tackled before we can count ourselves in the list of countries with the best healthcare plans.
The government hospitals in India are not in a good state as explained above. Less than 42% of urban and 46% of rural population opt for public healthcare services owing to various reasons explained above. There is a need for more budget allocation in health sector and subsidized rates at private hospitals. Political parties have to unite and have to share the same level of passion, to make UHC a reality; otherwise we will be stuck. There is a need for high level of commitment by the parties to invest in health. Ministries of Finance and Human Resources need to work closely with the Ministry of Health to achieve the target. There needs to be a massive brainstorm between varied institutions and organizations and not just institutions run by the government. There is a need to rope in nongovernmental and private organizations that can make suggestions on how to make the UHC plan stronger. We cannot replicate the healthcare plans of other countries, considering our demographics are very different. But we can take clues from other countries. While private sectors play an important role in contributing to health by providing umpteen services, the government needs to focus on adequate public funding to improve the quality of healthcare services.
Issue of Below Poverty Line (BPL)
Large numbers welfare schemes of government of India are for individuals who are “below poverty line” (BPL). Also, Ayushman Bharat Insurance Scheme covers a specific group of peoples. I am not the expert to elaborate on controversies about the criteria of defining below poverty line as this controversy is not only for India but even for other countries also. What I wish to point out that a huge population of India is though above the cutoff of below poverty line, but still they are poor enough to afford current cost of modern treatment in India. Though, they are out of benefit of many government health schemes. Another issue is rather peculiar. Many individual are actually above middle class category but still have BPL card and get benefit of government schemes though actually they are not eligible for the same.
Nephrology as a Speciality in India
Being a nephrologist, it will be unfair if I do not mention the status of nephrology care in India. I will only concentrate on chronic kidney disease (CKD), a public health issue and its last stage end-stage renal disease (ESRD), where patients need renal replacement therapy (RRT), which means maintenance dialysis, hemodialysis (MHD) or continuous ambulatory peritoneal dialysis (CAPD) or renal transplant (RT). About 8%–9% of adult Indian population suffers from CKD and approximately 4.0 lakh adult populations require RRT at any point of time. There is no need to stress that all the three treatments, MHD, CAPD, and RT, are costly and out of reach to common man and facilities for them are concentrated in bigger cities.
In spite of CKD having many common risk factors to other noncommunicable diseases (NCDs) and also a risk multiplier to other NCDs, till late CKD has not been given any recognition by policy makers as an important issue for the society. It is only when some VIPs get CKD and because of reporting in media of flourishing unrelated RT in the country that CKD got some importance. Some time back a separate national program for CKD was thought of, but then this idea was dropped by MOHFW, Government of India (personal communication).
There are 0.7 nephrologists per million population in India when compared to 0.1–53 nephrologists in the world[16] [Figure 13]. One can thus imagine that nephrologist alone cannot handle problem of CKD and ESRD, and as such we need active program for prevention of CKD and decreasing the load of patients with ESRD. However, CKD still is not taken as active component of NCD programs in India.

- Nephrologist workforce in countries with less than 1 nephrologist per million
In 2018, approximately 8000 RT was done in India with 90%–95% from living donor and 5%–10% from deceased donor. Deceased donor program in the country is very slowly developing and at present far from adequate. There are approximately 6000 patients on CAPD at any time. From the society point of view, CAPD is not a preferred therapy in the country. The very idea that a patient has to manage himself at home discourages a majority of patients to accept CAPD as preferred mode of therapy for ESRD.
Therefore, a majority of patients with ESRD opt or forced to opt MHD. In addition to requirement of infrastructure for MHD, hemodialysis machines, and water treatment plant, there is equal need of trained manpower performing MHD to patients. Home MHD is practically nil in the country. A majority of MHD is either provided by hospitals or standalone hemodialysis units. With nephrologist being decimally low in country, manpower for MHD has to come from trained non-nephrologist internist and trained dialysis nurses/technicians. For training internist for MHD physician, Indira Gandhi National Open University with Directorate General Health Services developed Post-Doctoral Certificate Course in Dialysis Medicine since 2011 [Figure 14]. However, after the first 2 years, the course had to be stopped apparently because there were not many takers of the course and also because of incoordination among different stakeholders. So, we are currently having acute shortage of non-nephrologist trained doctors who can supervise the dialysis units.

- Post-Doctoral Certificate in Dialysis Medicine advertisement
The second workforce required for the MHD is trained nurses or technicians. There are many states in India who are running courses to train nurses/technicians for MHD. There is also Paramedical Council existing in India, which is supposed to organize multiple paramedical courses, including course for dialysis technicians, but somehow the council has not able to produce trained manpower for MHD at national level.
Therefore, though Hon. Prime Minister had started National Dialysis program across country, with an aim to establish dialysis unit in every district of the country, in the absence of trained physicians for dialysis supervision and trained nurses/technician for conducting the MHD, time will tell the degree of success this program will have in coming future.
Finally, most patients in India are on the receiving end, and taken granted at least in public hospitals. It looks that illness is due to some fault of patient. Most cannot afford to take treatment as their right. One who asks relevant but more questions regarding illness or treatment is labeled as “irritating patient.” While on one side these patients do need minimal standard of care, on the other side doctors in public sector are working with many odds such as lack of infrastructure, manpower, facilities, and increasing expectations of patients. There is a need to have a balance between the two, for which policy makers have to work hard if violence against doctors is to be avoided in future.
In the end, one issue, which no government has ever touched, is the population of the country. Whatever progress we do, if the population goes on increasing with same pace, whether it is water, food, clean air, or health, all will become inadequate for our generations to come. In 2050, Indian population is expected to be 1.6 billion, much more than China [Figure 15]. Indians need to build a family by planning and not by chance.

- Population growth in India and China
For every lacuna in the system, a doctor is not to be blamed, and by no means any aggression against doctors is justified. It is the responsibility of lawmakers in the country that the rule of law should be upheld and doctors are allowed to do their duties fearlessly.
I will end by a quote from social media....

References
- The Declaration of Alma-Ata: International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September, 1978 ^ Preamble, WHO-UNICEF/CF/HST/1985- 034/Anx. 04/07
- National Health Profile 2018. Central Bureau of Health Intelligence. Directorate General Health Services. Ministry of Health and Family Welfare, Government of India
- [Google Scholar]
- Available from: https://www.who.int/gho/health_workforce/physicians_density/en/
- Available from: http://clinicalestablishments.gov.in/cms/Home.aspx
- The global nephrology workforce: Emerging threats and potential solutions! Clin Kidney J 2015:1-12.
- [Google Scholar]




