

Translate this page into:
Oxidative Stress in Peritoneal Dialysis Patients: Association with the Dialysis Adequacy and Technique Survival
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Increased oxidative stress is suggested as one of the possible mechanisms of structural and functional damage to the peritoneal membrane in peritoneal dialysis patients. But there are few available data on the association of oxidative stress with peritoneal dialysis adequacy and technique survival. The present study was undertaken to investigate the association of oxidative stress biomarkers with the peritoneal dialysis adequacy and technique survival.
Methods:
This prospective single-center observational study was conducted between January 2010 and May 2015. Adequacy of dialysis, malondialdehyde levels in the serum and erythrocytes (as an indicator of lipid peroxidation), the concentration of ceruloplasmin, transferrin, and sulfhydryl groups in the blood, and total peroxidase activity in erythrocyte (as indicators of antioxidant system) were determined in 44 stable ambulatory non-diabetic peritoneal dialysis patients.
Results:
The follow-up period was 3 years. We identified a negative correlation between the serum level of malondialdehyde in the patients and total weekly Kt/V. Peritoneal weekly CrCl was positively correlated with the levels of transferrin, total peroxidase activity, and SH– groups. Daily peritoneal ultrafiltration had a positive correlation with the total peroxidase activity and the serum transferrin levels. The results of the Kaplan–Meier analysis and the log-rank test also demonstrated a significant difference in the cumulative technique survival rate between the patients with ceruloplasmin level ≤0.19 g/l and ≥0.2 g/l.
Conclusions:
The results mentioned above could be considered as one of the ways to explain better technique survival in PD patients.
Keywords
Adequacy
technique survival
oxidative stress
peritoneal dialysis

Introduction
End-stage renal disease (ESRD) is a global health burden and the number of patients is considerably increasing from year to year.[12] In fact, in Ukraine, approximately 13% of ESRD patients are maintained on peritoneal dialysis (PD).[3] Despite significant advances in technique survival, the duration of PD therapy is still limited. There are several factors effecting PD technical survival: age, the presence of diabetes, renal residual function (RRF), glucose degradation products (GDP), and peritonitis.[4] In recent years, numerous studies have been devoted to the study of oxidative stress in PD patients, which is defined as an imbalance in production of free radicals and antioxidant activity.[567891011] So, at present, increased oxidative stress has been suggested as one of the possible mechanisms of structural and functional damage to the peritoneal membrane in long-term PD patients.[412]
Ignace et al. have revealed that a preserved RRF is associated with lower levels of oxidative stress markers in stable PD patients.[13] Morinaga et al. have demonstrated that the elevated effluent free radicals are associated with RRF and technique failure in stable PD patients. But, in general, there has been very little research on the topic devoted to the association between oxidative stress and PD adequacy. Thus, the present study was undertaken to investigate the association of oxidative stress biomarkers with PD adequacy and technique survival.
Materials and Methods
Study design and subjects
This prospective single-center observational study was conducted at State Institution “Institute of Nephrology of the National Academy of Medical Sciences” for between January 2010 and May 2015 in Kyiv, Ukraine. The study was carried out within the framework of the Institute's research work: “The Detection of New Prognostic Negative Determinants of Peritoneal Dialysis Survival and Possible Ways of Their Pharmacological Correction” (Domestic Trial Registration Number is 0117U002122). The study protocol was approved by the Ethics Committee of the Institute. Written informed consent was obtained from all the subjects participating in the study.
Forty-four PD outpatients (31 males, 13 females) were included in the study. All patients had been undergoing continuous ambulatory PD (CAPD) for more than 3 months. They were observed to determine the effect of oxidative stress on dialysis adequacy and technique survival. The observation period lasted 36 months.
The mean age of the patient population was 48.9 ± 13.2 years. All the patients received commercially available, glucose-based dianeal PD solution (Baxter Inc.) of various strengths (1.36%, 2.27%) and icodextrin. All recruited PD patients received four exchanges daily. The diabetics and the patients with a history of peritonitis or significant illness/hospitalization in the previous 3 months were excluded. The average duration of PD therapy at this study entry (at baseline) was 29 [18.5–37] months. All data were obtained during routine clinical practice, immediately after enrollment in the study. The patients took the medications including iron supplementation in 29/44 (66%), erythropoietins in 26/44 (59%), angiotensin-converting enzyme inhibitors/angiotensin receptor blockers in 21/44 (48%), and statins in 12/44 (27%).
Methods
Whole blood samples were collected from the patients after an overnight fast during the time of the routine outpatient visit. The blood samples were processed immediately after sampling. The routine biochemical parameters, including blood and daily dialysate concentration of urea, creatinine, serum albumin, C-reactive protein (CRP), cholesterol, and glucose were carried out using an automatic analyzer “Flexor junior” (Netherlands). The hematological parameters of blood were determined using “ABX Micros-60” (France).
The adequacy of dialysis was determined by measuring the total weekly creatinine clearance (CrCl) (it was normalized to 1.73 m2 of the body surface area) and total weekly urea clearance (Kt/V) using the Watson formula for body water. Peritoneal Kt/V and renal Kt/V were estimated separately. The dialysate/plasma creatinine ratio (D/P) was calculated by the concentrations of creatinine in the 24-h dialysate and the plasma.
Along with the standard diagnostic methods, we defined the malondialdehyde concentration in the serum (MDAs) and erythrocytes (MDAe) as an indicator of lipid peroxidation. Such parameters as the concentration of ceruloplasmin (CP), transferrin (TR), and sulfhydryl groups (SH– groups) in the blood and total peroxidase activity in erythrocyte (TPAe) were studied as the indicators of antioxidant system. In order to estimate MDA and TPA in erythrocytes, we used erythrocyte suspension which was drawn using vials containing 3.8% sodium citrate and centrifuged at 3000g for 10 min. Red cell mass was washed three times with isotonic sodium chloride and centrifuged at 3000g for 10 min.
MDA concentration
In this assay, the following reagents were used: tris (hydroxymethyl) aminomethane, tris (hydroxymethyl) aminomethane hydrochloride, malonaldehyde bis (diethyl acetal) (Sigma-Aldrich, USA), trichloroacetic acid, and thiobarbituric acid (Merck, Germany), hydrochloric acid, and potassium chloride (HLR, Ukraine). About 0.1 ml serum or red blood cells were added to 1.5 ml 0.025 M Tris-buffer with potassium chloride (pH 7.4) and incubated at 37°C for 30 min. About 1 ml 20% of trichloroacetic acid solution was added to the samples and centrifuged at 3000g for 15 min. Supernatants (2 ml) were added to 1 ml 0.8% of thiobarbituric acid solution and heated at 100°C for 10 min. The absorbance was measured using spectrophotometer Lambda 25 UV/vis (PerkinElmer, USA) at 532 nm and calculated using a molar extinction coefficient of 1.56 × 105/M/cm.[14] Malonaldehydebis (diethyl acetal) solution was used as standard. MDA concentration was expressed as μmol/l.
CP concentration
We used the following reagents: 1,4-phenylenediamine dihydrochloride, ceruloplasmin human, sodium fluoride (Sigma-Aldrich, USA), sodium acetate (Merck, Germany), and acetic acid (HLR, Ukraine). The experimental samples: About 0.05 ml of serum was added to 4 ml 0.4 of acetic buffer solution (pH 5.5) and 0.5 ml 0.5% aqueous solution of 1,4-phenylenediaminedihydrochloride. The control samples: About 0.05 ml of serum was added to 1 ml 3% of sodium fluoride solution, 4 ml of acetate buffer solution, and 0.5 ml 0.5% aqueous solution of 1,4-phenylenediaminedihydrochloride. The samples were incubated at 37°C for 1 h. Around 1 ml 3% of sodium fluoride solution was added to the experimental samples. The absorbance was measured using a spectrophotometer KFK-3-01 (ZOMZ, Russia) at 530 nm.[14] The human CP solution (Sigma-Aldrich, USA) was used as standard. CP concentration was expressed as g/l.
TR concentration
For this assay, we used ferric ammonium citrate (Sigma-Aldrich, USA) and TR (BioChemica, Fluka). About 0.2 ml of serum was added to 2 ml 0.2% of ammonium–iron (III)–citrate solution (pH 5.5–5.8). The absorbance was measured using a spectrophotometer Lambda 25 UV/vis (USA) at 440 nm.[14] TR concentration was calculated as the difference between the absorbance of the solution for 30 min. The human TR (BioChemica, Fluka) was used as standard. The result was expressed in g/l.
TPAe concentration
The TPAe was determined according to the following procedure.[14] We used the next reagents: indigo carmine (Sigma-Aldrich, USA), sodium acetate (Merck, Germany), acetic acid, hydrogen peroxide, and sulfuric acid (HLR, Ukraine). About 0.5 ml hemolysate of erythrocyte (1: 1000), 1 ml 0.2 M of acetate buffer (pH 4.9), and 1 ml 0.05 M of indigo carmine solution were incubated at 30°C for 5 min. The reaction started by the addition of 0.5 ml 0.03 M of hydrogen peroxide solution to the test samples. Then, 0.5 ml of distilled water to the control samples was added. The reaction stopped in 2 min by addition 3 ml 20% of sulfuric acid. The absorbance was measured using spectrophotometer KFK-3-01 (ZOMZ, Russia] at 670 nm. TPA of erythrocytes was expressed as μkat/g Hb.
The concentration of SH– groups
SH– groups in serum were determined according to the procedure.[14] For this assay, potassium iodide (Sigma-Aldrich, USA), iodine solution, sodium phosphate monosubstituted, bi-substituted, and starch (HLR, Ukraine) were used. About 0.05 ml of serum was dissolved in 0.5 ml of distilled water, and, then, 0.5 ml 6 M of potassium iodide solution, 2 drops of 5% starch solution, and 1.8 ml 0.1 M of phosphate buffer (pH 7.6) were added. The absorbance was measured using a spectrophotometer KFK-3-01 (ZOMZ, Russia) at 500 nm before and after the application of 0.3 ml 0.001 N of iodine solution. The SH– groups concentration was expressed as mmol/l.
Statistical analysis
Analysis and all graphs were performed using MedCalc (Belgium). The average means (M) and standard deviations (SD) or the median (Me) and interquartile ranges [Q25–Q75] were calculated according to a normal distribution. For the statistical analysis, we used Student's t-test and nonparametric (U-test) Mann–Whitney test. Categorical variables were expressed as proportions, and Chi-square tests were used for comparison of two groups. Pearson's or Spearman's (as appropriate) correlation tests were used to evaluate the association between oxidative stress biomarkers and PD adequacy parameters.
Survival curves were constructed according to the Kaplan–Meier method and compared using the log-rank test. Technique survival times were censored when patients died, underwent transplantation, transferred to HD transferred or were classified as “technique failures.” technique failure was defined as all reasons for PD withdrawal of PD. The duration of technique survival was calculated from the date of inclusion in the study. For this analysis, in January 2010, the patients were categorized into two groups according to baseline CP level. P values were calculated, and the null hypothesis was rejected if the P value was <0.05.
Results
The patients' characteristics are summarized in Table 1. We identified a significant negative correlation between the serum level of MDA in the patients and total weekly Kt/V [r = −0.68, P < 0.0001]. Moreover, the level of peritoneal weekly CrCl was positive and significantly correlated with the levels of TR [r = 0.38, P = 0.01], TPAe [r = 0.63, P < 0.0001] and SH– groups [r = 0.8, P < 0.0001]. Daily peritoneal ultrafiltration had a significant positive correlation with the TPA [r = 0.7, P < 0.0001] and the serum TR level [r = 0.56, P = 0.0001]. In addition, peritoneal Kt/V had a significant correlation with TPA [r = 0.37, P = 0.01]. D/P creatinine ratio was negatively correlated with TR level [r = −0.54, P = 0.02], but, it was positively correlated with TPA [r = 0.5, P = 0.005]. No significant correlations were found for the level of oxidative stress biomarkers with the patient urine volume and time on PD [Table 2].
| Parameters | Markers or Indicators |
|---|---|
| Clinical parameters | |
| Male gender (%) | 70.5 |
| Age (years) | 48.9±13.2 |
| Charlson Comorbidity Index (points) | 5.57±1.5 |
| BMI (kg/m2) | 27.4±3.9 |
| Serum albumin (g/l) | 36.8±13.2 |
| CRP (mg/l) | 9.8±3.3 |
| Systolic blood pressure (mmHg) | 137±14.2 |
| Diastolic blood pressure (mmHg) | 82±11.9 |
| Hb (g/l) | 106.7±19.6 |
| Cholesterol (mmol/l) | 5.2±1.2 |
| Glucose (mmol/l) | 5.4±0.6 |
| Ferritin (ng/ml) | 548 [368.5-842.8] |
| Peritoneal dialysis parameters | |
| Time on PD (months) | 29 [18.5-37] |
| Urine volume (ml/24 h) | 750 [400-1200] |
| D/P creatinine ratio | 0.72±0.09 |
| High-average transporters (%) | 47.8 |
| High transporters (%) | 52.2 |
| Icodextrin (%) | 11.4 |
| Total Kt/V | 1.78 [1.62-2.54] |
| CrCl (l/1.73 m2) | 58.2±17.7 |
| Daily peritoneal ultrafiltration (ml) | 600 [400-830] |
| Oxidative stress parameters | |
| MDAs (µmol/l) | 372.9 [295.8-450] |
| MDAe (µmol/l) | 591.6 [488.7-694.4] |
| CP (g/l) | 0.09 [0.07-0.1] |
| TR (g/l) | 1.16 [0.6-2.05] |
| TPA (µkat/g Hb) | 1.82±0.4 |
| SH- groups (mmol/l) | 2.41 [2.12-3.14] |
BMI: Body mass index, CP: Ceruloplasmin, CrCl: Creatinine clearance, CRP: C-reactive protein, Hb: Hemoglobin, MDAs: Serum malondialdehyde, MDAe: Erythrocytes malondialdehyde, total Kt/V: Total weekly Kt/V urea, TR: Transferrin, TPA: Total peroxidase activity, SH- groups: Sulfhydryl groups
| PD adequacy parameters | Oxidative stress biomarkers | |||||
|---|---|---|---|---|---|---|
| MDAs | MDAe | CP | TR | TPA | SH- groups | |
| Time on PD |
r=0.25 P=0.32 |
r = −0.09 P=0.71 |
r = −0.43 P=0.05 |
r = −0.48 P=0.04 |
r = −0.08 P=0.75 |
r = −0.24 P=0.56 |
| Urine volume |
r=0.39 P=0.11 |
r=0.27 P=0.14 |
r = −0.13 P=0.56 |
r=0.32 P=0.19 |
r=0.02 P=0.9 |
r=0.55 P=0.10 |
| D/P creatinine ratio |
r=0.003 P=0.99 |
r=0.05 P=0.8 |
r = −0.11 P=0.62 |
r = −0.54 P=0.02 |
r=0.5 P=0.005 |
r = −0.006 P=0.98 |
| Total Kt/V |
r = −0.68 P < 0.0001 |
r=0.03 P=0.9 |
r=0.36 P=0.11 |
r=0.36 P=0.14 |
r = −0.22 P=0.53 |
r = −0.53 P=0.11 |
| Peritoneal Kt/V |
r = −0.13 P=0.6 |
r = −0.07 P=0.44 |
r=0.31 P=0.16 |
r=0.19 P=0.45 |
r=0.37 P=0.01 |
r = −0.19 P=0.65 |
| Renal Kt/V |
r = −0.36 P=0.13 |
r=0.5 P=0.03 |
r = −0.04 P=0.85 |
r=0.21 P=0.39 |
r = −0.14 P=0.55 |
r = −0.05 P=0.88 |
| Peritoneal CrCl |
r=0.08 P=0.57 |
r=0.1 P=0.48 |
r=0.28 P=0.22 |
r=0.38 P=0.01 |
r=0.63 P < 0.0001 |
r=0.8 P < 0.0001 |
| Daily peritoneal ultrafiltration |
r=0.42 P=0.08 |
r = −0.01 P=0.99 |
r=0.56 P=0.0001 |
r = −0.45 P=0.06 |
r=0.7 P < 0.0001 |
r = −0.26 P=0.47 |
CP: Ceruloplasmin, CrCl: Creatinine clearance, MDAs: Serum malondialdehyde, MDAe: Erythrocytes malondialdehyde, PD: Peritoneal dialysis, total Kt/V: Total weekly Kt/V urea, TR: Transferrin, TPA: Total peroxidase activity, SH- groups: Sulfhydryl groups
Oxidative stress and PD technique survival
During the 3-year follow-up, 9 of 44 (20.5%) patients dropped out from PD, including 4 (9.0%) patients who died and 4 (9.0%) patients who transferred to hemodialysis. 7 patients were considered to be “technique failures,” but they continued PD treatment for various reasons: the inability to formation of an adequate vascular access 3 (6.8%), the patient's refusal to transfer to hemodialysis 2 (4.5%), and noncompliance 2 (4.5%).
In the Cox proportional hazard model, among all the studied oxidative stress markers, CP level was found to be an important factor influencing PD technique survival (P = 0.019) [Table 3]. According to this adjusted for age, gender, Charlson comorbidity index, CRP level and iron use model, and the hazard ratio (HR) of PD technique, failure was 8.8 fold higher in the patients with the blood CP level ≥0.2 g/l.
| Variables | Parameter estimation | SE | χ2 | P | HR (95% CI) |
|---|---|---|---|---|---|
| MDAs | 0.2 | 0.4 | 1.94 | 0.62 | 1.5 (0.3; 7.5) |
| MDAe | 0.67 | 0.48 | 1.94 | 0.16 | 3.87 (0.57; 26.1) |
| CP | 0.88 | 0.23 | 9.37 | 0.002 | 8.8 (2.2; 35.7) |
| TR | -0.9 | 0.5 | 3.28 | 0.07 | 0.16 (0.02; 1.1) |
| TPA | 0.37 | 0.06 | 0.37 | 0.55 | 2.09 (0.18; 23.7) |
| SH- groups | 0.34 | 0.18 | 2.3 | 0.09 | 1.3 (0.17; 6.8) |
SE: Standard error, HR: Hazard ratio, 95% CI: 95% confidence interval; χ2=Chi-square, Results in bold indicate a significant finding
The average serum CP level in 28 patients of the “technique survival” group was significantly higher compared with 15 patients of the “technique failure” group 0.26 [0.22–0.32] g/l versus 0.09 [0.07–0.1] g/l, P < 0.0001, Figure 1]. No significant differences were found in the clinical outcomes between 2 groups stratified according to CP levels, excluding PD technique survival [Table 4]. The results of the Kaplan–Meier analysis and log-rank test also demonstrated that there was a significant difference in the cumulative technique survival rate between the patients with CP level ≤0.19 g/l and CP level ≥0.2 g/l [log-rank test: χ2 = 11.3, P = 0.0008, Figure 2].
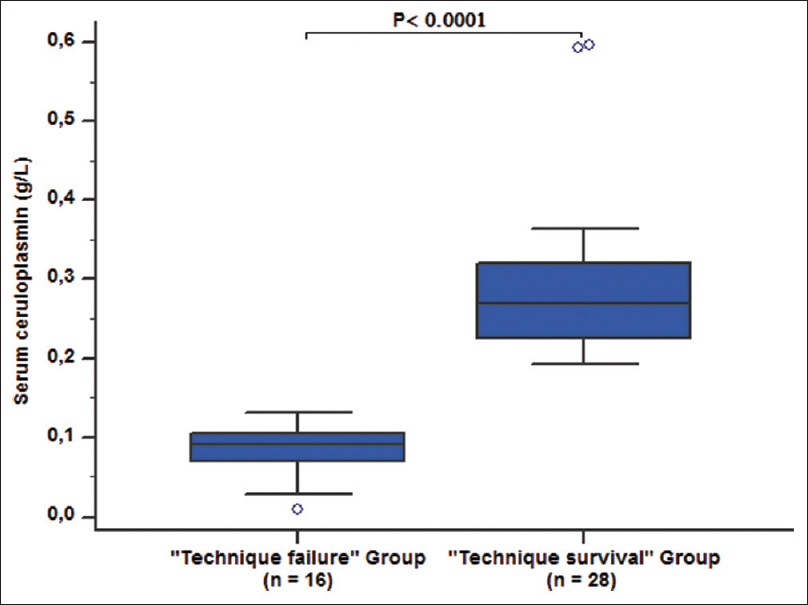
- Serum levels of ceruloplasmin in the studied groups on the left side: “technique failures” group (n = 16), on the right side: “technique survival” group (n = 28); P < 0.0001
| Outcomes | Total (n=44) | Ceruloplasmin levels (g/l) | P | |
|---|---|---|---|---|
| ≤0.19 (n=26) | ≥0.2 (n=18) | |||
| Events [n (%)] | ||||
| Death | 4 (9.0%) | 3 (11.5%) | 1 (5.5%) | 0.8 |
| Transfer to HD | 4 (9.0%) | 4 (15.4%) | 0 | 0.2 |
| Technique survival | 28 (63.6%) | 12 (46.2%) | 16 (88.8%) | 0.001 |
| PD-related infection | 9 (20.5%) | 4 (15.4%) | 5 (27.7%) | 0.54 |
| Cardiovascular events | 11 (25%) | 7 (27.0%) | 4 (22.2%) | 0.9 |
| Admissions/patient-year (95% CI) | ||||
| Hospitalizations rate | 0.2 (0.13-0.29) | 0.22 (0.13-0.35) | 0.17 (0.07-0.3) | 0.51 |
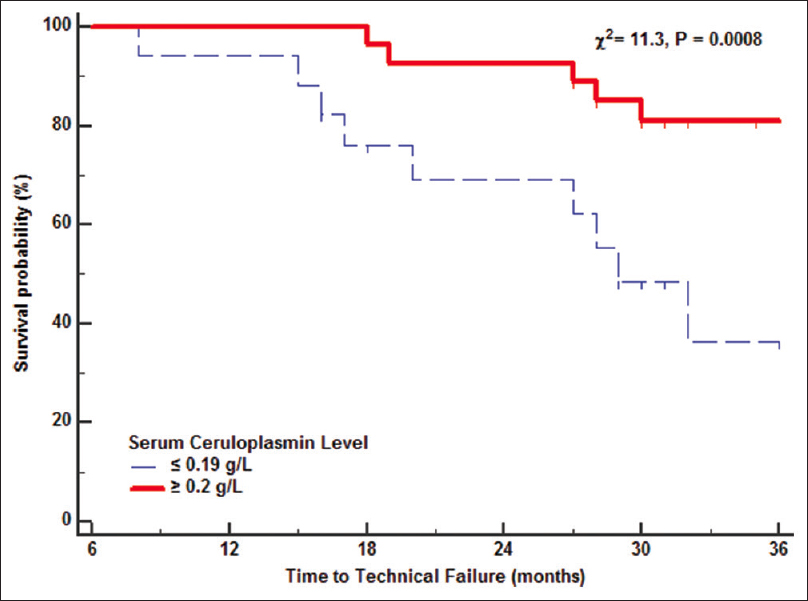
- Kaplan–Meier technique survival (death censored) curves in PD patients dichotomized according to the serum ceruloplasmin level in the 3-year follow-up. Dotted line: Serum ceruloplasmin level ≤0.19 g/l; solid line: serum ceruloplasmin level ≥0.2 g/l (χ2 = 11.3, P = 0.0008)
Discussion
In our study, we investigated the association between the oxidative stress biomarkers and parameters of PD adequacy. Our results have confirmed the numerous scientific data that PD patients suffer from increased oxidative stress.[5612] As well as the majority of previous studies,[58910] we have demonstrated an imbalance between pro- and antioxidant capacities in CAPD patients, namely: An increase in MDA and a decrease of antioxidants (CP, TR, TPA, and SH– groups).
To our knowledge, it follows that this is the first study demonstrating a close link between the oxidative stress parameters and the PD adequacy. In our view, a special attention deserves a direct association between the blood indicators of antioxidant activity and peritoneal weekly CrCl level in PD patients. In addition, we first reported on the effect of CP levels on PD technique survival. Ignace et al. also investigated the association between oxidative stress and PD adequacy. In this study, renal Kt/V and total weekly Kt/V were strongly associated with serum lipid hydroperoxides and MDA levels after adjustment for sex, inflammation, and nutritional factors.[13] But, in contrast to us, they investigated only blood MDA level and found no association with peritoneal clearance.[13]
Numerous studies have highlighted the strong linkage between preservation of residual renal function (RRF) and oxidative stress.[131516] Furuya et al. showed that PD patients with preserved RRF (>300 ml/day) had significantly higher plasma levels of advanced oxidation protein products compared with PD patients with daily urine volume less than 300 ml/day.[15] Morinaga et al. demonstrated that circulating free radicals were significantly and inversely associated with RRF in PD patients.[16] The authors concluded that RRF preservation reduced oxidative stress in PD patients. On the contrary, in the present study, we found no significant associations between oxidative stress biomarkers level and daily urine volume.
In our study, we demonstrated that plasma antioxidant levels were more related with the adequacy and PD technique survival than with the end product of peroxidation. It is of importance to note that our findings are in accordance with the report by Montazerifar et al.[17] The authors showed that decreased activity of enzymatic antioxidant defense system played a leading role in accelerated atherogenesis in PD patients.
It must be stressed that the main findings of the present study were the strong association of the antioxidant system indicators (CP, TR, SH– groups, and TPA) in the blood with the PD adequacy parameters and a significantly higher level of all-cause PD technique failure in patients with CP level ≤0.19 g/l at baseline. In addition, the prognostic value of CP level was confirmed by the Cox model analysis. In this connection, two topical questions are raised: (1) Why serum CP is decreased in PD-patients? (2) How can a low level of serum CP affect the peritoneal membrane?
Numerous studies have been lately published on the significance of both oxidative and antioxidant functions of CP in the genesis of various pathological conditions. It has been shown that an increase in serum CP is associated with a high cardiovascular risk in chronic kidney disease patients,[18] in patients with acute coronary syndromes,[19] heart failure,[20] and diabetic nephropathy.[21] Besides, CP has been reported to be related to schizophrenia[22] and several types of cancer.[23] At the same time, decreased serum CP level; have been demonstrated in patients with liver fibrosis, chronic hepatitis,[24] and neurodegenerative disease.[25] Thus, the mechanisms lead to a decrease or an increase in the level of CP in different diseases. But they have not been fully studied xidative stress under the same conditions.
It is well established that CP is a multioxidase with both pro-oxidant and anti-oxidant properties.[26] Its prooxidant functions are mainly related to amine oxidase and NO oxidase activities.[27] Multiple antioxidant effects of CP are realized through the following functions: the conversion of reactive Fe2+ into Fe3+ (form bound in TR),[2829] destruction of oxygen free radicals,[29] and inhibition of neutrophil myeloperoxidase oxidant activity.[30]
In our study, CP was primarily considered as ferroxidase. This was the reason why we determined the blood CP level using the spectrophotometric method. This method allowed us to estimate precisely ferroxidase activity of CP, that is, its antioxidant effects. In our view, the fact of a decrease in ferroxidase activity of CP in PD patients and its correlation with the dialysis adequacy is explained by PD solutions' uses which contain dextrose as an osmolyte, lactate as a buffer, and different electrolytes, including chloride.[31]
Considering the fact that most patients included in the present study (89%) received commercial glucose-containing PD fluids, the low-serum CP level might be mediated by the following mechanisms: (1) an increase in oxidative status due to the accumulation in the peritoneum of GDP with formation of free radicals, and[32] (2) the presence of chloride in the abdominal cavity (96 mmol/l in each 1000 ml of dianeal PD solution)[31] whereas its presence is not found in other pathological conditions.
Thus, the reason of our conclusions stems from the results published clinical and experimental studies. In the first place, it has been demonstrated that the oxidative stress intensity and the level of tissue injury in the peritoneum can depend on an imbalance in the production of free radicals and antioxidant activity.[32] Chronic exposure to glucose-containing PD solution leads to hydrogen peroxide (H2O2) generation and the mesothelial cells are damaged.[3233] In agreement with these conclusions, Morinaga et al. have reported that the elevated levels of effluent free radicals predict death-censored technique failure in stable PD patients.[16] The authors observed a significant direct correlation between the levels of effluent carbon-centered free radicals and effluent 8-hydroxy-2′-deoxyguanosine at baseline, the latter being a known marker of oxidative stress in peritoneal effluent.[34] In turn, it can promote the initiation of free radical reactions based on the physiological functions of CP, its deacreased ferroxydase activity and untimely utilization of Fe2+. It should be noted that the inhibition of CP can be increased due to the low level of pH in the peritoneum.[35] In this context, the high intraperitoneal production of free radicals with a low level of local CP might be one of the causes of PD technique failure.
Accordingly, concerning the role of chloride in reducing the antioxidant capacity of CP, our hypothesis is based on the following scientific data. Herlihy et al. demonstrated that 125 mM chloride potentiated human fibrocyte differentiation in vitro.[31] Cox et al. hypothesized that elevated serum concentration of NaCl, observed at least for a few hours after eating a high-salt meal, could contribute to fibrosis.[36] But the chloride concentration in PD fluid was lower than those of serum. So, the authors have concluded that the chloride concentration in PD fluid could not be directly responsible for PD fluid potentiation of fibrocyte differentiation.[31] On the other hand, chloride ions are able to suppress the ferroxidase activity of CP, especially in low pH conditions.[37] As a result, the level of Fe2+ is increased and leads to the stimulation of free radical reactions under elevated levels of H2O2. The formation of active oxygen metabolites contributes to the blood lipids and proteins damage with the formation of their degraded and oxidized forms. The latter leads to a decrease in the cell membranes functions, including the peritoneal membrane.[32]
We acknowledge limitations in our study. In this study, the oxidative stress markers were measured once. Thus, establishment of cause and effect relationship between these parameters was not quite correct. Moreover, a modest number of non-diabetic clinically stable patients and total absence of low transporters could affect the reproducibility of our results. In addition, there was a high probability of changes in the intensity of oxidative processes in PD patients with infectious or noninfectious complications of PD.
Nevertheless, our results have provided an initial understanding of the relationship between PD adequacy and a patient's antioxidant status. Our study has demonstrated that a decreased level of the blood CP is a significant predictor of technique failure in PD patients. Data for this trial may also lead to a larger scale study assessing the effect of antioxidants therapy on PD adequacy and technique survival.
Conclusions
In summary, we have found that increased serum MDA level, an end product of the lipid peroxidation, is associated with inadequate PD, whereas the normal levels of blood antioxidant parameters are associated with a sufficient dose of dialysis, peritoneal clearance, and daily ultrafiltration. Baseline serum CP level is an independent predictive factor for PD technique survival. The changes of oxidative stress pathways due to CP could be one of the explanations of PD technique survival failure. Further well-designed, randomized controlled clinical trials with antioxidants are required to establish their potential for improving PD adequacy and technique survival.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors have no competing interests to declare. Although Baxter Healthcare is a provider of peritoneal dialysis therapy in our hospital, that fact has no influence on the study results.
References
- Early chronic kidney disease: Diagnosis, management and models of care. Nat Rev Nephrol. 2015;11:491-502.
- [Google Scholar]
- Peritoneal dialysis as a first versus second option after previous haemodialysis: A very long-term assessment. Int J Nephrol. 2014;2014:693670.
- [Google Scholar]
- Renal replacement therapy in Ukraine: Epidemiology and international comparisons. Clin Kidney J. 2014;7:330-5.
- [Google Scholar]
- Inflammation and the peritoneal membrane: Causes and impact on structure and function during peritoneal dialysis. Mediators Inflamm. 2012;2012:912595.
- [Google Scholar]
- Oxidative stress in patients treated with continuous ambulatory peritoneal dialysis (CAPD) and the significant role of vitamin C and E supplementation. Int Urol Nephrol. 2013;45:1137-44.
- [Google Scholar]
- Comparison of markers of oxidative stress, inflammation and arterial stiffness between incident hemodialysis and peritoneal dialysis patients – An observational study. BMC Nephrol. 2009;10:8.
- [Google Scholar]
- Oxidative stress during peritoneal dialysis: Implications in functional and structural changes in the membrane. Kidney Int. 2006;69:2022-8.
- [Google Scholar]
- Antioxidant status of patients on peritoneal dialysis: Associations with inflammation and glycoxidative stress. Perit Dial Int. 2009;29:89-101.
- [Google Scholar]
- The importance of oxidative stress in patients with chronic renal failure whose hypertension is treated with peritoneal dialysis. Cell Biochem Funct. 2011;29:249-54.
- [Google Scholar]
- Markers of inflammation and oxidative stress in peritoneal dialysis: A comparison between high and low peritoneal transporters. J Nephrol. 2010;23:453-8.
- [Google Scholar]
- Lipid peroxidation and antioxidants in continuous ambulatory dialysis patients. Perit Dial Int. 1992;12:252-6.
- [Google Scholar]
- Long-term exposure to new peritoneal dialysis solutions: Effects on the peritoneal membrane. Kidney Int. 2004;66:1257-65.
- [Google Scholar]
- Preserved residual renal function is associated with lower oxidative stress in peritoneal dialysis patients. Nephrol Dial Transplant. 2009;24:1685-9.
- [Google Scholar]
- Intensity of oxidative stress and activity of angiotensin converting enzyme in blood of patients with uncomplicated pyelonephritis. Ukr Biochem J. 2017;89:99-105.
- [Google Scholar]
- Impact of residual renal function on plasma levels of advanced oxidation protein products and pentosidine in peritoneal dialysis patients. Nephron. 2009;112:c255-61.
- [Google Scholar]
- Effluent free radicals are associated with residual renal function and predict technique failure in peritoneal dialysis patients. Perit Dial Int. 2012;32:453-61.
- [Google Scholar]
- Effect of peritoneal dialysis on antioxidant defense system and oxidative stress. Hong Kong J Nephrol. 2012;14:33-7.
- [Google Scholar]
- Plasma ceruloplasmin, a regulator of nitric oxide activity, and incident cardiovascular risk in patients with CKD. CJASN. 2014;9:462-7.
- [Google Scholar]
- Acute phase proteins and systolic dysfunction in subjects with acute myocardial infarction. J Thromb Thrombolysis. 2008;26:196-202.
- [Google Scholar]
- Low serum ferroxidase I activity is associated with mortality in heart failure and related to both peroxynitrite-induced cysteine oxidation and tyrosine nitration of ceruloplasmin. Circ Res. 2014;114:1723-32.
- [Google Scholar]
- Serum ceruloplasmin level as a predictor for the progression of diabetic nephropathy in Korean men with type 2 diabetes mellitus. Diabetes Metab J. 2015;39:230-9.
- [Google Scholar]
- Plasma copper, iron, ceruloplasmin and ferroxidase activity in schizophrenia. Schizophr Res. 2006;86:167-71.
- [Google Scholar]
- Ceruloplasmin as a prognostic marker in patients with bile duct cancer. Oncotarget. 2017;8:29028-37.
- [Google Scholar]
- Serum ceruloplasmin levels correlate negatively with liver fibrosis in males with chronic hepatitis B: A new noninvasive model for predicting liver fibrosis in HBV-related liver disease. PLoS One. 2013;8:e77942.
- [Google Scholar]
- Does ceruloplasmin defend against neurodegenerative diseases? Curr Neuropharmacol. 2018;16:1-10.
- [Google Scholar]
- Structure to function relationships in ceruloplasmin: A “moonlighting” protein. Cell Mol Life Sci. 2002;59:1413-27.
- [Google Scholar]
- Ceruloplasmin is a NO oxidase and nitrite synthase that determines endocrine NO homeostasis. Nat Chem Biol. 2006;2:486-93.
- [Google Scholar]
- Labile iron pool: The main determinant of cellular response to oxidative stress. Mutat Res. 2003;531:81-92.
- [Google Scholar]
- Ceruloplasmin (ferroxidase) oxidizes hydroxylamine probes: Deceptive implications for free radical detection. Free Radic Biol Med. 2012;53:1514-21.
- [Google Scholar]
- Ceruloplasmin is an endogenous inhibitor of myeloperoxidase. J Biol Chem. 2013;288:6465-77.
- [Google Scholar]
- Peritoneal dialysis fluid and some of its components potentiate fibrocyte differentiation. Perit Dial Int. 2015;36:367-73.
- [Google Scholar]
- Oxidative stress in patients undergoing peritoneal dialysis: A current review of the literature. Oxid Med Cell Longev. 2017;2017:3494867.
- [Google Scholar]
- Cultured rat mesothelial cells generate hydrogen peroxide: A new player in peritoneal defense? J Am Soc Nephrol. 1996;7:2371-8.
- [Google Scholar]
- Increased susceptibility to oxidant-mediated tissue injury and peritoneal fibrosis in acata-lasemic mice. Am J Nephrol. 2008;8:661-8.
- [Google Scholar]
- Protection of ceruloplasmin by lactoferrin against hydroxyl radicals is pH dependent. Biochem Cell Biol. 2012;90:397-404.
- [Google Scholar]
- Modulation of the redox state of the copper sites of human ceruloplasmin by chloride. J Protein Chem. 1995;14:611-9.
- [Google Scholar]




