

Translate this page into:
Fetuin-A, inflammation, and coronary artery calcification in hemodialysis patients
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Hemodialysis patients have extremely increased cardiovascular mortality. Vascular calcification, inflammation, and low serum fetuin-A levels are implicated for increased mortality. In this study, relationship between coronary artery calcification, inflammation, and serum fetuin-A levels were investigated. Seventy-eight hemodialysis patients (38 male, 40 female, mean age: 52±14.5 years) were included. All patients were on dialysis for more than 6 months. Coronary artery calcium scores (CACS) are determined by electron-beam computed tomography. Serum CRP, IL-1β, IL-6, TNF-α, and serum fetuin-A levels were measured. Mean CACS value was 488.5±94.5. Serum fetuin-A levels were negatively correlated with CACS (r:–0.30, P=0.009). Patients are divided into two groups according to total CACS value; group 1 (CACS<10), group 2 (CACS≥10). There was a statistically significance difference in fetuin-A levels between CACS group 1 and group 2 (P=0.001). In this study, serum fetuin-A levels were associated with total CACS. This Fetuin-A may play a role in increased mortality in this group of patients via facilitating CAC.
Keywords
Fetuin-A
hemodialysis
inflammation
vascular calcification

Introduction
The most common cause of death in dialysis patients is cardiovascular disease (CVD). When compared with general population, CVD in patients with end stage renal disease (ESRD) is 10-20 times higher despite recent developments in renal replacement therapies (RRT).[1] This can be attributed to many factors including advanced age, atherosclerosis, endothelial dysfunction (ED), hypertension, anemia, hyperparathyroidism, chronic inflammation, diabetes, and its macro-microvascular complications, left ventricular hypertrophy (LVH, malnutrition and vascular calcification (VC). Coronary artery calcification (CAC) is a part of extended state of VC which can be detected even in early decades of patients with ESRD.[2] This may be contributing to premature CVD and markedly increased mortality in patients with ESRD. The presence of VC (including CAC) appears to correlate with impaired calcium-phosphorus metabolism that can be extensively seen in patients with ESRD. However, there were no spectacular changes in VC with the use of calcium containing phosphate binders in this population. Therefore, additional clinical factors such as advanced age, vitamin D therapy, dialysis vintage, and cellular factors rather than only a passive process due to calcium-phosphate deposition in the vessel wall.[3] This suggests that VC is an orchestrated event that can be attributed to programmed process regarding both active inflammation and osteogenesis at vascular level. The coronary artery calcification score (CACS) in uremic patients receiving hemodialysis reflects the severity of atherosclerotic vascular disease and predicts the cardiovascular events.[45]
Fetuin-A is a hepatocyte-derived serum protein (molecular weight, ~60 kD). Serum concentrations are relatively high with levels between 0.5 and 1.0 g/l in average populations. Fetuin-A is an inhibition of calcification, limiting hydroxyapatite crystal formation.[3]
In the present study, we aimed to investigate the relationship between fetuin-A, inflammation markers such as interleukin (IL) 1β, IL-6, TNF-α, and CRP and coronary artery calcification in patients with ESRD receiving hemodialysis.
Patients and Methods
Patients
This was a cross-sectional study involving ESRD patients who had been on hemodialysis for at least 6 months in Hemodialysis Unit of Istanbul University Istanbul School of Medicine, Istanbul, Turkey. Exclusion criteria included (i) congestive heart failure, (ii) the presence of active infections, (iii) autoimmune disease, (iv) primary hyperparathyroidism, (v) calcium supplements, calcium containing phosphate binders, and vitamin D treatment. Out of a total of 108 patients, 6 patients had congestive heart disease with the clinical evidence of heart failure (NYHA class III-IV), 4 patients had active infections, 3 patients had primary hyperparathyroidism, 5 patients had autoimmune disease and 12 patients had valvular heart disease. None of the patients had arrhythmia based on ECG. Four patients were on non-calcium containing phosphate binder therapy. None of our patients were taking calcium-containing phosphate binders.
Remaining 78 (38 women, 40 men) patients were enrolled in the study. Hemodialysis modality includes conventional 4-h HD three times a week with polysulfone dialysers. A 250 ml/min (range 200-300 ml/min) of mean blood flow rate was obtained during dialysis sessions. Dialysate fluid composition includes 140 mEq/l of sodium, 1-4 mEq/l of potassium, 3 mEq/l of calcium, 1.8 mEq/l of magnesium, and 33 mEq/l of bicarbonate. Urea (Kt/V) values were calculated by Daugirdas second generation formula.[6] Demographic data, medications, primary cause of ESRD and dialysis duration were recorded. Systolic and diastolic blood pressures were measured on the non-fistula arm in an upright sitting position after at least 5 min of rest using an Erka sphygmomanometer (PMS Instruments Ltd, Berkshire, UK) of appropriate cuff size. Two readings were recorded for each individual, and the average was defined as the subject's blood pressure. Patients with systolic and diastolic blood pressure above 140 and 90 mmHg, respectively, or those receiving antihypertensive medications were assumed as hypertensive.
Thirty patients were on treatment with antihypertensive drugs (13 of them on angiotensin-converting enzyme (ACE) inhibitors, 12 of them receiving angiotensin receptor blocker (ARB) and 5 of them both receiving Calcium channel blocker and ACE inhibitors.
The study protocol was approved by the institutional medical ethics committee of Istanbul University and written informed consent was obtained from all subjects included in the study.
Venous blood samples for biochemical analyses were drawn after an overnight fast between 8:00 p.m. and 8:00 a.m. at a single midweek dialysis session. All biochemical analyses including glucose, creatinine, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and plasma triglyceride concentrations were performed by an oxidase-based technique at Roche/Hitachi Modular System (Mannheim, Germany) in the Central Biochemistry Laboratory. Serum fetuin-A (Biovender Research and Diagnostic Products), interleukin (IL) 1β (Biosource Europe S.A. Belgium), IL-6 (Biosource Europe S.A. Belgium) and TNF-α (Biosource Europe S.A. Belgium) levels were performed via ELISA kit method (Biotech Instruments ELx800).
Coronary artery calcium scoring (CACS) was performed by a 16-MDCT scanner (Sensation 16, Siemens Medical Solutions, Erlangen, Germany). CACS were calculated by as described by Agatston et al.,[5] A calcification was defined as a minimum of two adjacent pixels (>0.52 mm2) with a density over 130 Hounsfield units. The peak intensity (in Hounsfield unit) and area (in square millimeter) of the individual calcifications were calculated. Scores were obtained by multiplying each area of interest by a factor indicating peak density within the individual area. Image quality and scoring accuracy were assessed by one radiologist who carefully made vessel-byvessel and calcific focus-by-calcific focus inspections of each image. The radiologist was blinded to the clinical and laboratory results of the patients. The intraobserver coefficient of variation for CACS was 2.5%.
The statistical analysis was carried out by the Statistical Package for Social Sciences for Windows ver. 15.0 (SPSS Inc., Chicago, IL, USA). Datawere expressed as the mean±SD, with a significance level of P<0.05. For dichotomous variables, the frequency of positive occurrences were givenalong with their corresponding percentages. Statistical comparisons of individual groups were based on Student's t-test for continuous variables whereas the correlations between groups were evaluated by Spearman test.
Significant determinants (age, URR, Kt/V, fetuin-A, uric acid, TNF-α, and hypertension) identified from this analysis were studied in a stepwise multiple regression model.
Results
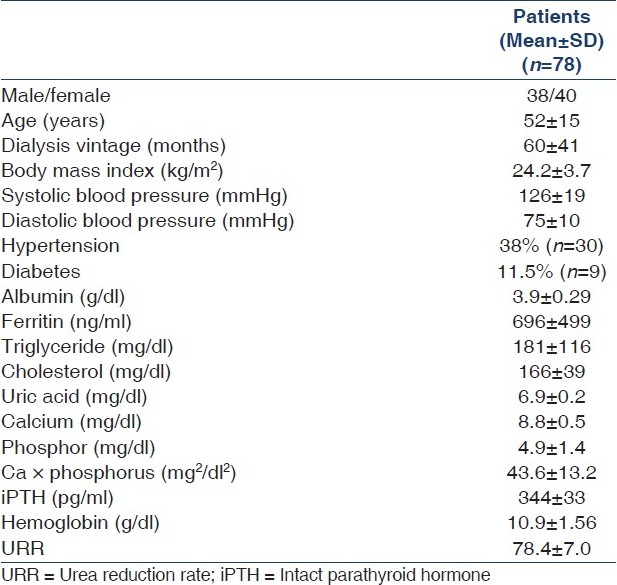
Demographic, clinical characteristics and biochemical parameters, fetuin-A levels, inflammation parameters, and CAC scores of the patients are depicted in Table 1. The etiology of the ESRD patients include diabetic nephropathy (n=9), chronic glomerulonephritis (n=15), hypertensive nephropathy (n=30), polycystic kidney disease (n=7), nephrolithiasis (n=13), and unknown (n=4).
Mean CACS value of 78 hemodialysis patients was 488.5±94.5. Patients were divided into two groups according to total CACS value; group 1 (CACS<10), group 2 (CACS≥10) [Table 2]. CACS was associated with increased age, BMI, and decreased URR and Kt/V [Table 2]. Serum fetuin-A levels were negatively correlated with log of total CACS (r2: 0.50) [Figure 1]. There was a statistically significant difference in fetuin-A levels between total CACS group 1 and group 2 (P=0.001).


- Relationship between fetuin-A and log of the total coronary artery calcification scores
A significant association was found between total CACS and TNF-α. There was no relationship between CACS and other inflammation markers (hs-CRP, IL-1β, IL-6) [Table 2].
Logistic regression analysis to determine independent predictors of total CACS including patient's age, serum uric acid, fetuin-A and TNF-α levels, URR, Kt/V and being hypertensive are detailed in Table 3. In the stepwise analysis, patients age and fetuin-A levels were found to be independent predictors of CACS≥10.

Discussion
The main finding of this cross-sectional study was that the extent of coronary artery calcification detected by multidetector computed tomography in HD patients is associated with patients age, BMI, Kt/V, fetuin-A, and TNF-α level.
Coronary artery calcification score is regarded as an index of the severity of atherosclerotic vascular disease; helps to anatomically assess the coronary artery disease and may also predict future adverse cardiovascular events, especially in ESRD patients.[7] Fetuin-A, is one of the inhibitor of soft tissue and vascular calcification. There are conflicting results about relationship between fetuin-A levels and CACS in ESRD patients. As previously mentioned in hemodialysis population there is a significant correlation between serum fetuin-A and CACS of ESRD patients.[8–12] However, Hermans et al. showed no difference between ESRD and healthy subjects when compared according to their serum fetuin-A levels[13] and Mehrotra et al.,[14] demonstrated an association between fetuin-A levels and a calcification in non-dialyzed patients with diabetic nephropathy. In the present study, we found an inverse relationship between total CACS and fetuin-A levels. In subgroup analysis according to levels of CACS, age and fetuin-A were statistically and independently significant between CACS group 1 and group 2 when a stepwise fashion of logistic regression analysis was used. Our results are consistent with previous studies that demonstrated negative correlations with VC and fetuin-A.[1516]
Some inflammation markers such as hs-CRP, IL-6 and fibrinogen have been found to be associated with atherosclerosis in ESRD patients.[17–19] However, Caliskan et al.,[15] found no correlation between hs-CRP levels and CACS. In our study there was no correlation between total CACS and IL-1β, CRP, and IL-6. An association was seen with TNF-α, but in the stepwise analysis, it was not found an independent predictor of CACS. Thus, beyond the effect of inflammation, the role of serum fetuin-A levels in vascular calcification may be far more complex than previously thought.[16] The differences may be consistent with a different pathogenetic role of fetuin-A in different stages of chronic renal disease.[14] Additionally, to assess the relationship between vascular calcification and serum fetuin-A levels in a cross-sectional study may be difficult, as vascular calcification is a slowly progressive process and serum fetuin-A levels may fluctuate, possibly dependent on flares of inflammation.
The other risk factor associated with increased CACS in ESRD patients is advanced age.[3] In the present study, age was found to be a predictor of CACS. This finding could be attributed to increased plaque burden and inflammation with aging.
Hypertensive patients are more prone to atherosclerosis and vascular calcification.[20] Jensky et al., recently demonstrated that different measures of BP are associated with significant calcification in multiple vascular beds and that these associations vary with age.[21] In our study, hypertensive patients were on antihypertensive medications including ACE-inhibitors, ARBs and CCB and hypertension is not found a predictor of CACS in multiple regression analysis. Possibly, limited number of hypertensive patients might play a role in this finding in our study.
In conclusion, our study investigated a larger population not limited to diabetic ESRD patients. In the present study we found a negative relationship between fetuin-A levels and total coronary artery calcification scores. This result is consistent with the other results obtained in different studies.[15] Our study has some limitations; first, this is a cross sectional analysis of ESRD patients regarding vascular calcification and fetuin-A. Second, the sample size was relatively small. Another potential limitation is that computed tomography cannot determine whether calcium is in the intima or media of the arterial wall. Since this is not a prospective controlled study we can not draw cause and effect relations from our findings. Further experimental and clinical studies are needed to determine the exact relationship between factors that induce and inhibit vascular calcification.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Arterial medial calcification in end-stage renal disease: Impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18:1731-40.
- [Google Scholar]
- Molecular determinants of vascular calcification: A bench to bedside view. Curr Mol Med. 2006;6:515-24.
- [Google Scholar]
- Coronary artery calcification is related to coronary atherosclerosisin chronic renal disease patients: A study comparing EBCT-generated coronary artery calcium scores and coronary angiography. Nephrol Dial Transplant. 2004;19:2307-12.
- [Google Scholar]
- Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15:827-32.
- [Google Scholar]
- Second generation logarithmic estimates of single-pool variable volume Kt/V: An analysis of error. J Am Soc Nephrol. 1993;4:1205-13.
- [Google Scholar]
- Electron beam computed tomographic coronary calcium scanning: A review of guidelines on use in asymptomatic persons. Mayo Clin Proc. 1999;74:243-52.
- [Google Scholar]
- Association of low Fetuin-A (AHSG) concentrations in serum with cardiovascular mortality in patients on dialysis: A cross-sectional study. Lancet. 2003;361:827-33.
- [Google Scholar]
- Low Fetuin-A levels are associated with cardiovascular death: Impact of variations in the gene encoding fetuin. Kidney Int. 2005;67:2383-92.
- [Google Scholar]
- Associations of serum Fetuin-A with malnutrition, inflammation, atherosclerosis and valvular calcification syndrome and outcome in peritoneal dialysis patients. Nephrol Dial Transplant. 2005;20:1676-85.
- [Google Scholar]
- Role of calcification inhibitors in the pathogenesis of vascular calcification in chronic kidney disease (CKD) Kidney Int. 2005;67:2295-304.
- [Google Scholar]
- Cardiac calcifications: Fetuin-A and other risk factors in hemodialysis patients. ASAIO J. 2006;52:150-6.
- [Google Scholar]
- Study on the relationship of serum Fetuin-A concentration with aortic stiffness in patients on dialysis. Nephrol Dial Transplant. 2006;21:1293-9.
- [Google Scholar]
- Serum Fetuin-A in nondialyzed patients with diabetic nephropathy: Relationship with coronary artery calcification. Kidney Int. 2005;67:1070-7.
- [Google Scholar]
- Coronary artery calcification and coronary flow velocity in haemodialysis patients. Nephrol Dial Transplant. 2010;25:2685-90.
- [Google Scholar]
- Association among serum Fetuin-A level, coronary artery calcification, and bone mineral densitometry in maintenance hemodialysis patients. Artif Organs. 2009;33:844-54.
- [Google Scholar]
- Strong association between malnutrition, inflammation and atherosclerosis in chronic renal failure. Kidney Int. 1999;55:1899-911.
- [Google Scholar]
- Tumor necrosis factor-α promotes in vitro calcification of vascular cells via the cAMP pathway. Circulation. 2000;102:2636-42.
- [Google Scholar]
- Carotid artery calcification and atherosclerosis at the initiation of hemodialysis in patients with end-stage renal disease. Clin Nephrol. 2010;73:360-9.
- [Google Scholar]




