

Translate this page into:
Comparison of glomerular filtration rate estimated by plasma clearance method with modification of diet in renal disease prediction equation and Gates method
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Glomerular filtration rate (GFR) prediction equations are widely used in clinical practice for quick assessment of kidney function. Gates method using radionuclide technique is an alternative to prediction equations for quick assessment of GFR. Aim of the study was to compare Gates method and modification of diet in renal disease (MDRD) equation in a sizeable patient population with wide range of renal function to evaluate their clinical utility. GFR was estimated in 897 subjects with wide range of renal function by gates method, and MDRD equation and results were compared against measured GFR. Subjects were divided in to 4 groups (0-30 ml, 31-60 ml, 61-90 ml, >90 ml) on the basis of measured GFR and comparison between two methods done through linear regression analysis. Analysis of R2 indicated that 56% of the interindividual variability for Gates GFR was in accordance to variation in measured GFR, in the GFR range of (0-30 ml), this value dropped to 39% in the GFR range of 31-60 ml, 40% in the GFR range of 61-90 ml, 26.4% in the GFR range of >90 ml, the corresponding figure for MDRD GFR were 47.9%, 31.1%, 17.6% and 16.1%, respectively. Gates method is more precise for GFR estimation at all levels of renal function.
Keywords
Gates method
GFR measurement
MDRD equation
Tc99m–DTPA

Introduction
Glomerular filtration rate (GFR) is considered to be the best parameter to assess the overall kidney function.[1] GFR can be measured by calculating the plasma clearance of various glomerular filtration markers like inulin, ethylene-diamine-tetra-acetic-acid, diethylene-triamine-penta-acetic acid (DTPA), iothalamate and iohexol.[2] Although, the plasma clearance methods give accurate GFR measurement but these methods are time consuming and require timed blood sampling.[34] However, the the modification of diet in renal disease (MDRD) equation, a serum creatinine based equations for GFR prediction is widely used to estimate GFR, but the intrinsic limitations of serum creatinine in estimation of GFR is well known.[1] As an alternative to these equations, techniques using radioisotopes have also been developed for instant assessment of GFR. These methods do not require urine or blood collection and results can be obtained within few minutes. The method introduced by Gates is the most commonly used method.[5] There is paucity of study to show the relative superiority of Gates method and MDRD equation for estimation of GFR. Therefore, we undertook this study to compare the Gates method and MDRD equation in a sizeable patient population with wide range of renal function to evaluate their clinical utility.
Materials and Methods
Subjects
Eight hundred ninety-seven subjects (485 male, 412 female) ranging on age from 18 to 70 years were included in the study from October 2004 to September 2006. Informed consent was obtained from all patients before the test. The GFR was estimated by plasma clearance method, Gates method and MDRD equation in all patients.
GFR estimation by Gates method
All the subjects of the study were asked to report in the morning, minimum 1 hour prior to the initiation of the study. They were asked to drink 5 ml/kg plain water on arrival and were provided a comfortable environment to wait. GFR estimation by Gates method and GFR ‘measurement’ by plasma clearance method was performed in the day and utilized the same injection of filtration marker Tc99m-DTPA.
Tc99m-DTPA was prepared in our hospital using a commercially available freeze-dried kit (Board of Radioisotope Technology, Mumbai, India). The dose of 37 MBq (1 mCi) was administered intravenously under the gamma camera and transit of tracer through the kidneys was recorded. Gates method estimates total and individual kidney GFR from the integral activity accumulated by each kidney during 120-180 seconds after injection, assuming that all the glomerular filtrate produced post-injection is in transit through the nephrons and has not yet left the kidney. The administered dose of Tc99m-DTPA was calculated with pre and post-injection counting of the syringe over the camera. GFR values were calculated using a computerized gamma camera (Orbiter 75, Siemens, Erlangen, Germany) equipped with low energy all-purpose collimator. Renal region of interest (ROI) and semilunar background ROI, were drawn at the inferior pole of the kidney avoiding the liver, spleen and iliac vessels in all frames of the dynamic study to obtain time-activity curves. GFR was calculated, starting from renal uptake during 2-3 min period after injection, corrected for background activity, linear attenuation and depth (the distance was estimated on the basis of body height and weight). The background curve was multiplied by each side to intersect the renal curve 120 seconds after the rise in kidney activity: The area subtended by the relative kidney function curve between 120 and 180 seconds, corrected for the background curve, and defined the total renal counts. To calculate quantitative GFR values, the total counts were normalized with regard to the injected activity dose and time interval. The resulting values are defined as clearance equivalent and were converted to individual and total quantitative renal clearance values expressed in ml/min. The quantitative GFR is obtained multiplying the regression coefficient (9.75621) by the total renal uptake percent subtracting the intercept value (6.1983) used in the Gates method.
GFR estimation using MDRD equation
GFR was also predicted from serum creatinine level using the following simplified MDRD equation.[6]
GFR = 186 × (S. Cr)–1.154 × (age)–0.203 × (0.742 if patient is female)
The serum creatinine was measured on same day by an autoanalyzer (RA 1000, Bayer, Ireland).
GFR measurement by clearance method
For obtaining the ‘measured’ GFR, plasma clearance of Tc99m-DTPA was calculated by obtaining two venous blood samples at 60 and 180 minute postinjection of Tc99m-DTPA. Radioactivities in the samples were counted using a γ-well counter and glomerular filtration rate was calculated using Russell's algorithm by a computer-assisted program.[7] Obtained GFR values were corrected for height and weight (body surface area) and results were expressed in milliliter per minute per 1.73 square meter body surface area. The calculated GFR was used as the measured GFR.
All subjects were divided in to 4 groups according to level of kidney function (0-30, 31-60, 61-90, >90 ml) on the basis of ‘measured’ GFR and for each group descriptive statistics has been calculated. The GFR by plasma clearance method was considered Gold standard in this study. The GFR estimated by clearance method was compared from GFR estimated by Gates method and MDRD equation. The comparison between Gates method and MDRD equation was also done. The precision of the test was defined by square of the regression coefficient determined by linear regression analysis.
Statistical analysis
Pearson's correlation was used to see the correlation between the different tests. For the comparison of two methods, standard linear least square regression analysis was used; P-value of 0.05 or less in the regression analysis was considered significant. The SPSS version 12 was used for the statistical analysis.
Results
The patient characteristics and indications for estimating GFR are shown in Table 1. The mean age, gender ratio, height, weight, serum creatinine, GFR estimated by Gates and MDRD equation are shown in Table 2, with all subjects divided in to 4 different levels of GFR (0-30, 31-60, 61-90, >90 ml) measured by clearance method.

The comparative differences of correlation coefficient and precision of GFR estimated by all three methods are shown in Table 3. Analysis of correlation between clearance method and Gates method indicated 56% correlation with the measured GFR for the GFR range of 0-30 ml, and correlation went down to 39% in the GFR range of 31-60 ml, 40% in the GFR range of 61-90 ml, 26.4% in the GFR range of >90 ml. Analysis of correlation between clearance method and MDRD equation indicated the correlation of 47.9% with the measured GFR for the GFR range of 0-30 ml, and correlation went down to 31.1% in the GFR range of 31-60 ml, 17.6% in the GFR range of 61-90 ml, 16.1% in the GFR range of >90 ml. Overall, there was significant correlation between measured GFR and GFR estimated by gates method (r=0.73, P=0.001) [Figure 1] and the correlation was also significant between measured GFR and GFR estimated by MDRD equation (r=0.62, P=0.001) [Figure 2].

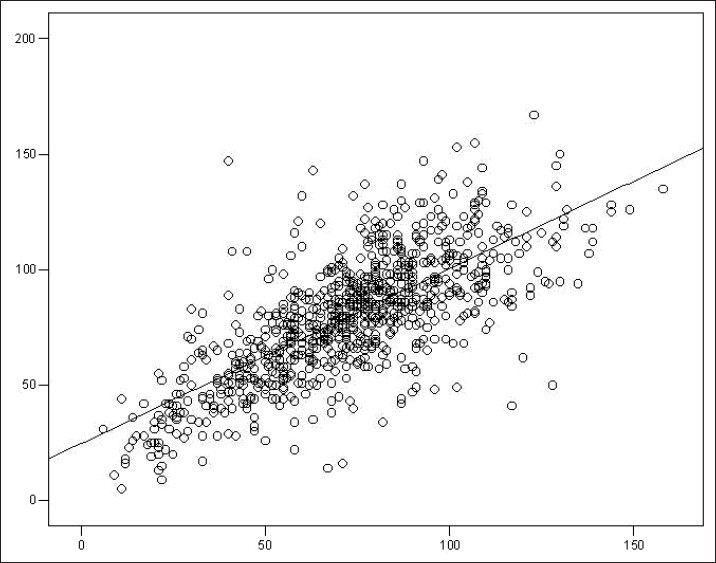
- Correlation between Gates GFR and measured GFR

- Correlation between MDRD-GFR and measured GFR
On linear regression analysis with depended variable GFR estimated by clearance method and predictable variable GFR by Gates method, the precision of the Gates method was 0.315 for GFR 0-30 ml, 0.152 for GFR 31-60 ml, 0.167 for 61-90 ml and 0.07 for GFR >90 ml. The precision of the MDRD equation was 0.230 for GFR 0-30 ml, 0.097 for GFR 31-60 ml, 0.031 for 61-90 ml and 0.026 for GFR >90 ml, respectively. Regression analysis showed that both Gates method and MDRD equation overestimated GFR at lower range of renal function and underestimated at higher range of renal function.
Discussion
The main finding of this study is the better correlation of Gates GFR with ‘measured GFR’ compared to MDRD GFR for all level of renal function. Our results also indicate that both Gates method and MDRD equation overestimates GFR at lower level of renal function and underestimates at higher level of kidney function. This current study revealed few important differences with the existing literature.[89] First, our study shows precision of Gates method decreases with increase in level of GFR which means Gates method will produce more reliable result at lower level of renal function i.e., lower GFR. Similar trend was observed for MDRD equation, where the obtained correlation was 0.479 for GFR range of 0-30 ml as against 0.161 for >90 ml range. MDRD equation was derived from patients of chronic kidney disease and is known to perform better at lower level of renal function.
A review of literature yielded limited number of studies in English, which have compared Gates method with a creatinine-based GFR prediction equation. De Santo et al.[8] evaluated GFR in 65 individual (15 healthy controls and 50 patients with renal disease) by Tc99m-DTPA renogram (Gates method), creatinine clearance (measured and predicted by Cockroft and Gault, CG) and by inulin clearance. They concluded that Gates method for GFR assessment is less precise than measured and predicted creatinine clearance. Itoh et al.[9] studied 133 patients (69 males and 64 females; age range 24-84 years) with a wide range of renal function and determined GFR simultaneously by γ-camera uptake method (Gates method), predicted creatinine clearance method (Cockcroft-Gault, CG) and single or two-plasma sample and concluded that Gates method is even less precise than the Cockcroft-Gault prediction equation. Both of our above findings are in contrast with the study of De Santo et al. and Itoh et al.[89] However, in both these studies Cockcroft-Gault equation was used to predict GFR rather that MDRD equation, which is presently, favored over Cockcroft-Gault equation as per recent National Kidney Foundation guidelines.[1] Aydin et al. compared measured GFR by single plasma sample methods (SPSMs), γ-camera Gates, 24-h endogenous creatinine clearance, and prediction equations [Cockcroft-Gault and MDRD] with the two plasma sample method (TPSM) considered as the reference in 115 potential kidney donors with normal renal function. They concluded that Gates method, creatinine clearance, Cockcroft-Gault prediction equation and MDRD prediction equation overestimated GFR (bias 5.76, 15.49, 13.24 and 6.72, respectively). The correlation coefficients were 0.49, 0.27, 0.48 and 0.43 for Gates method, creatinine clearance, Cockcroft-Gault prediction equation and MDRD prediction equation respectively.[10] Another recent multicentric study by Virga et al. has evaluated the performance of 12 different creatinine (Cr)-based equations commonly used to estimate GFR in predicting total Cr clearance (totCrCL) in 355 peritoneal dialysis patient and concluded that the Gates, Virga and 4-MDRD equations showed the best global performance.[11]
Apart from the difference in the prediction equation used, there are other issues involved with method of creatinine measurement. In the present study and the study by Itoh et al. creatinine measurement was done using an autoanalyzer; however, the method of creatinine measurement has not been mentioned in the study of De Santo et al.[89] It is well known that autoanalyzer produces more accurate measurement of creatinine than the conventional alkaline-picrate method.[1] Moreover, all these three studies were performed in three entirely different racial population. The study of De Santo et al. was performed in Caucasian population whereas the study of Itoh et al. was performed in Japanese population and the present study was done exclusively in Indian population. This also raises the issue of suitability of one GFR prediction equation for all racial groups. Number of subjects recruited in these two studies was also relatively small of 65 and 133, respectively. The study by De Santo et al. utilized inulin clearance as measured GFR, where as Itoh et al. used single sample Tc99m-DTPA clearance in 116 of 133 subjects recruited and the two-sample Tc99m-DTPA clearance was used only in 17 patients. In the present study, GFR was measured by two-sample Tc99m-DTPA clearance method in all subjects. The differences in study design might have influenced the results.
Serum creatinine concentration is the most widely used biochemical parameter to assess renal function. However, it is not an ideal marker of GFR, because apart from excretion by glomerular filtration, a significant portion is secreted by the renal tubules.[1213] Moreover, there is a small fraction of extra renal elimination of creatinine, which can become the major route of elimination in advanced renal insufficiency. Hence, an isolated serum creatinine measurement will overestimate GFR and this degree of overestimation is unpredictable.[1415] A concern with GFR prediction equations has been the bias from a lack of standard calibration in serum creatinine assays across laboratories.[1617] Presently there is no standard calibration for serum creatinine measurement for laboratories in India much like in the rest of the world. The implication was that a constant calibration bias caused greater inaccuracies in estimated GFR for persons with a normal serum creatinine level than that for persons with an elevated serum creatinine level.[1819] Other potential sources of measurement error include intraindividual variability in serum creatinine, racial and intraindividual variability in GFR, and intra-assay variability in creatinine and GFR measurement.
The clearance of Tc99m-DTPA in timed plasma collections is a very accurate method to measure the GFR and correlates very closely with inulin.[18–20] However, these methods are lengthy and time-consuming. The estimation of GFR by the Tc99m-DTPA renogram is proposed as an answer to the need of the simplicity without losing the precision.[521] Several sources of errors in the estimation of GFR by scintigraphy are recognized: Background correction, decay statistics, attenuation correction, and estimation of arterial plasma activity, system dead time, volume measurements and radiopharmaceutical quality. Of these, the bias for overestimation for GFR by the gates may be attributable to insufficient background correction.[22]
Conclusions
Gates method provides better estimate of GFR at all levels of renal function compared to MDRD equation. However, poor correlation exhibited by both this method with reference radionuclide clearance method makes them suboptimal for clinical use.
Source of Support: Nil
Conflict of Interest: None declared.
References
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1-266.
- [Google Scholar]
- How to assess glomerular function and damage in humans. J Hypertens. 1999;17:309-17.
- [Google Scholar]
- 99Tcm-DTPA for the measurement of glomerular filtration rate. Br J Radiol. 1976;49:794-6.
- [Google Scholar]
- Comparison of inulin, iothalamate, and 99mTc-DTPA for measurement of glomerular filtration rate. J Nucl Med. 1976;17:317-20.
- [Google Scholar]
- Glomerular filtration rate: Estimation from fractional renal accumulation of 99mTc-DTPA (stannous) AJR Am J Roentgenol. 1982;138:565-70.
- [Google Scholar]
- A simplified equation to predict glomerular filtration rate from serum creatinine (Abstract) J Am Soc Nephrol. 2000;11:A0828.
- [Google Scholar]
- Measurement of glomerular filtration rate: Single injection plasma clearance method without urine collection. J Nucl Med. 1985;26:1243-7.
- [Google Scholar]
- Measurement of glomerular filtration rate by the 99mTc-DTPA renogram is less precise than measured and predicted creatinine clearance. Nephron. 1999;81:136-40.
- [Google Scholar]
- Comparison of methods for determination of glomerular filtration rate: Tc-99m-DTPA renography, predicted creatinine clearance method and plasma sample method. Ann Nucl Med. 2003;17:561-5.
- [Google Scholar]
- Comparison of glomerular filtration rate measurements with the two plasma sample and single plasma sample, gamma camera Gates, creatinine clearance, and prediction equation methods in potential kidney donors with normal renal function. Nucl Med Commun. 2008;29:157-65.
- [Google Scholar]
- Comparison between creatinine-based equations for estimating total creatinine clearance in peritoneal dialysis: A multicentre study. Nephrol Dial Transplant. 2010;25:262-9.
- [Google Scholar]
- The relationship between endogenous creatinine clearance and serum creatinine in renal failure. Scand J Clin Lab Invest. 1964;16:273-80.
- [Google Scholar]
- Conventional measurement of renal function utilizing serum creatinine, creatinine clearance, inulin and para-aminohippuric acid clearance. Curr Opin Nephrol Hypertens. 1995;4:505-9. discussion 503-4
- [Google Scholar]
- Measured creatinine clearance from timed urine collections substantially overestimates glomerular filtration rate in patients with liver cirrhosis: A systematic review and individual patient meta-analysis. Nephrol Dial Transplant. 2005;20:1617-22.
- [Google Scholar]
- Recommendations for improving serum creatinine measurement: A report from the Laboratory Working Group of the National Kidney Disease Education Program. Clin Chem. 2006;52:5-18.
- [Google Scholar]
- Impact of standardized calibration on the inter-assay variation of 14 automated assays for the measurement of creatinine in human serum. Clin Chem Lab Med. 2005;43:1227-33.
- [Google Scholar]
- Predictive performance of renal function equations for patients with chronic kidney disease and normal serum creatinine levels. J Am Soc Nephrol. 2002;13:2140-4.
- [Google Scholar]
- Simultaneous measurement of renal clearance and plasma clearance of 99mTc-labelled diethylenetriaminepenta-acetate, 51Cr-labelled ethylenediaminetetra-acetate and inulin in man. Clin Sci (Lond). 1984;66:613-9.
- [Google Scholar]
- Utility of radioisotopic filtration markers in chronic renal insufficiency: Simultaneous comparison of 125I-iothalamate, 169Yb-DTPA, 99mTc-DTPA, and inulin. The Modification of Diet in Renal Disease Study. Am J Kidney Dis. 1990;16:224-35.
- [Google Scholar]
- Comparison of inulin, iothalamate, and 99mTc-DTPA for measurement of glomerular filtration rate. J Nucl Med. 1976;17:317-20.
- [Google Scholar]
- Reproducibility of three methods of renal clearance estimation without blood samples by means of 99mTc-DTPA. Contrib Nephrol. 1987;56:77-81.
- [Google Scholar]
- Influence of the background activity region selection on the measurement of glomerular filtration rate using the Gates method. Vojnosanit Pregl. 2008;65:729-32.
- [Google Scholar]




