

Translate this page into:
A multicenter cross-sectional study of mental and physical health depression in MHD patients
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Depression is ranked fourth among the disabling diseases affecting people worldwide and is the most common psychological problem in patients with End Stage Renal Disease (ESRD). The aim of this study is to assess the physical and emotional health status of renal dialysis patients, based on the SF-36 scale in relation to their economic status. Sixty maintenance hemodialysis patients, with a mean age of 40±13 years were included in this cross-sectional study using the SF-36 scale. It comprises 36 questions regarding physical and mental functions, body pain, vitality, etc. An SF-36 score of 50 or less was considered as moderate to severe depression and 51–100 as mild depression to good health. 56.81% of the patients who are below poverty line under dialysis had moderate to severe depression with regard to their health status. A physical health score of up to 50 was seen in 63.63% of patients below poverty line 63.63% (P= 0.16). A mental health score of 0–50 was observed in 61.63% of the cohort studied (P = 0.22). Among the patient with diabetes (28.33%) 55.56% had depression. Dialysis duration was directly associated with deteriorating physical health status and inversely proportional to their mental health status (P<0.05). There are problems in other regular activities due to depressed physical and mental health. The factors that were identified in this study that influence depression such as poverty status, increasing age, vintage and frequency of dialysis and treatment with erythropoietin dosage should be addressed and treated accordingly to improve the quality of life. Improving self-esteem with fruitful employment opportunities, concerted rehabilitation by professionals and easing of economic burden by private–public partnership is an achievable goal.
Keywords
Depression
hemodialysis
SF–36

Introduction
In India, there is an increasing incidence and prevalence of End Stage Renal Disease (ESRD) which is due to diabetes and hypertension. More than 90% of the patients with renal failure die within months of diagnosis because of inaccessibility of Renal Replacement Therapy (RRT) and cost.[1] The life expectancy in India on an average is 66.46 years. For males, it is 65.46 years and 67.57 years for females. The GDP growth rate in India is 8.80%, that is, US$1050 per person per year, where a value below US$11.71 at urban and US$7.73 at rural is below poverty line in the year 2010.
Depression has been recognized as a common treatable problem among dialysis patients that adversely affect their outcome. The syndrome of clinical depression consists of the presence of constellations of symptoms that include anhedonia, feelings of sadness, guilt, helplessness, hopelessness, etc. accompanied by changes in sleep, appetite, and libido. Delayed sleep onset, frequent awakening, restlessness, daytime sleepiness, spontaneous arousals are prevalent.[2] Patients’ perceptions of their health status help doctors and nurses to evaluate the effectiveness and introduce innovations in care. Though depression has been clearly demonstrated to predict mortality in a variety of medical conditions, there has not been any consistency about the association between depression and risks of mortality.[3–6]
This prospective cross-sectional study was performed to assess the physical and emotional health status of dialysis patients based on the SF-36 scale in relation to their economic status at the dialysis unit at Pondicherry Institute of Medical Sciences and TANKER Foundation at Chennai, India.
Materials and Methods
Sixty stable maintenance hemodialysis (MHD) patients from two centers in South India for a minimum of two months had consented for screening of depression and SF-36 scale and were enrolled in this cross-sectional study that was carried out from 01.05.2010 to 30.06.2010.Patients who are willing for the study, not critically ill, deaf or mentally retarded were included in the study; Continuously sleep-deprived patients, those not willing or comatose patients were excluded from the study.
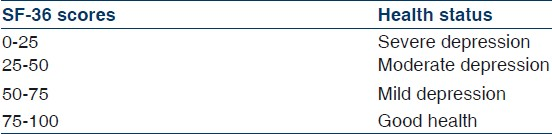
Physical and mental health is broadly affected by his/her social functioning, vitality, emotional role, physical functioning, social role, physical health, and body pain. SF-36 rates them and in this study of depression their physical and mental health is projected. Table 1 SF-36 is a non disease-specific instrument that describes health in a multidimensional way.[78] SF-36 consists of 36questions about the patient's quality of life comprising the ability to carry out daily activities and whether he feels troubled by ill health. The questions are being answered by choosing the best of the given alternatives. Data were entered in the in-built SF-36 questionnaire-guided computer program. Compiled data are presented in the form of distribution, percentage, and SF-36-scoringmethods. Statistical test EPI6 and Odds ratio were applied to assess the significance of the study findings. Each health item such as vitality, physical functioning, mental health score is assessed separately and a total score was given from 0–100 by the inbuilt computer system according to which the depression status is assessed.
Data on socio demographic variables, economic status, dialysis vintage, hemoglobin level, other associated co morbid conditions like Myocardial Infarction (MI) and diabetes mellitus, physical and emotional status, erythropoietin dosage, frequency of dialysis, age, BMI were assessed to find out the correlation with their depression level both physically and mentally.
Table 2 Shows the demography and results among our study subjects on dialysis. On comparing the demographic variables of this study that had a sample size of 60, 55% of the patients with ESRD had moderate to severe depression with regard to physical and mental health status. Depression was significant among females (P <0.001). There were equal numbers of people from both urban and rural areas. Below the poverty line, individuals showed statistical significance in relation to depression (P <0.001).
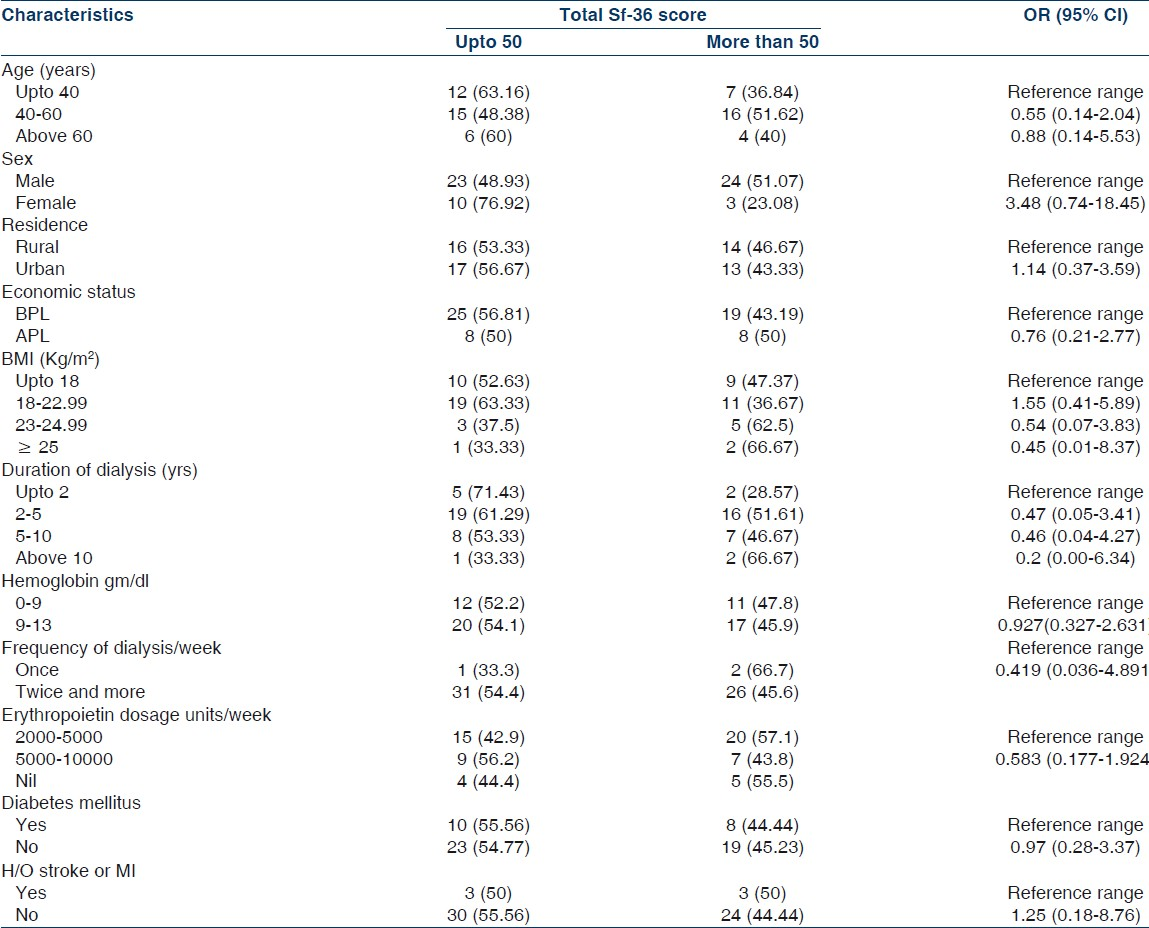
BMI and hemoglobin were uniform in their respective groups. Sixty percent of the elderly population above 60 years of age and 63.13% below 40 years showed moderate to severe depression. Financial status also played a role in the depression level of the study subjects as 56.81% below poverty line subjects were moderately to severely depressed{0.76 OR}. Past history of diabetes was present in 55.56% of patients and this was significantly associated with depression.
Fifty-seven percent of patients with vintage of dialysis less than 5 years were depressed (57.14%). Limitation in physical activities and other regular activities performed was seen in 69.41% of study subjects. Dialysis for a longer period was directly associated with deteriorating physical health status among study subjects and inversely proportional to their mental health status.
The physical health score up to 50 in BPL patients are 63.63% and their mental health score is 61.36%, which states high prevalence of depression [Figure 1]. Duration of dialysis is related to physical health score (P = 0.05).
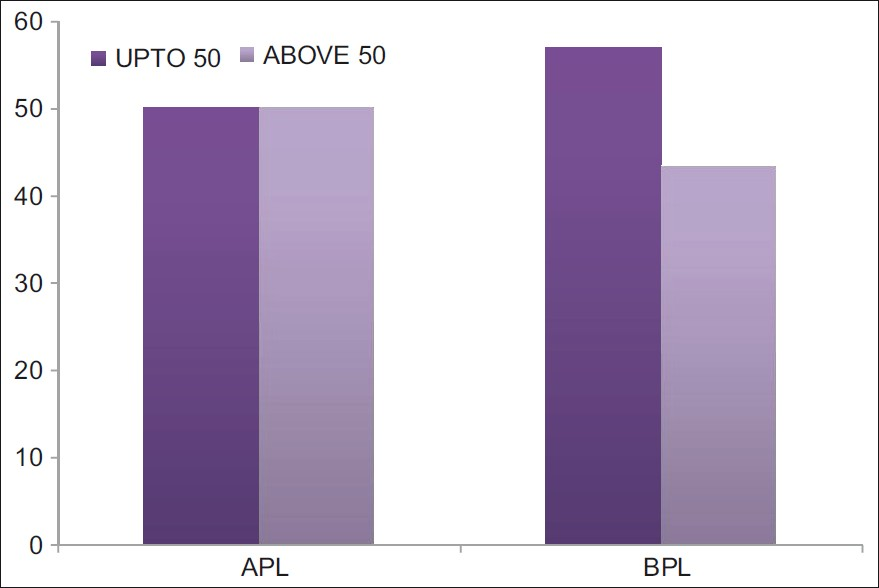
- The Bar graph shows the number of patients depressed, score upto 50% in each groups - above poverty line (APL) and below poverty line (BPL)
Table 3 shows that there were no significant statistical differences in the mean score of the physical function, social function, vitality, physical and mental health, and general health among the categorical variables in association with depression. This may be due to a limited statistical power due to a small sample size.

Figure 2 shows the average score of each health component such as vitality (46.53), physical health (46.93), general health (47.48), mental health (50.64), physical function (54.67), body pain (56.38), and social function (62.30) on X-axis. Y-axis shows their respective P values. Vitality (46.53), body pain (56.38), and social function (62.30) have a linear relationship as shown in the graph. The points closer to this line are physical health (46.93)and the mental health (50.64)that are shown to influence the obtained result by adding on to an increase in depression status if the physical and mental health is weak and the points farther away are general health and physical functioning that does not have much influence on the result.

- Shows a scatter diagram of the score of each health component
The vintage of dialysis showed significant P value (P = 0.027). The presence of diabetes was significant (P = 0.003) with depression. In this study, 28% of the patients were diabetic. A past history of coronary artery disease (CAD) was also statistically significant (P <0.001) with depression. Statistically significant associations were found in the performance of regular activities due to prevailing physical health status (P = 0.007) along with a decrease in the amount of time spent on such activities (P = 0.007). Body pain was also a limiting factor leading to depression but was not statistically significant. Mental health score was significant (P = 0.03). Gender in association with mental health score shows homogeneous values but gender shows a significant P value in association with the physical health score (P = 0.02). Other variables such as hemoglobin and BMI, when reduced due to ill health, were associated with depression of physical health.
Discussion
Chronic kidney disease in Asia is predominantly due to diabetes and hypertension and is rising in prevalence.[1] Depression is ranked fourth among disabling disease affecting the people worldwide and is the most common psychological problem in patients with ESRD. The prevalence of depression is 0–100% among dialysis population.[2] In the database of Fresenius Medical Care in the United States, Lowrie et al. have demonstrated that dialysis patients with scores lower than 51 on the mental component scale of the Sf-36 have progressively increasing risk of death.[3] In fact, patients with scores 0–37 have twice the relative risk of death than patients with scores of 51 or higher.[4] The impact of psychological factors on the outcome of patients with ESRDs has been receiving more attention recently.
In the present study, 55% of the patients with ESRD had moderate to severe depression with regard to physical and mental health status that was comparable to the studies from United States that have reported that incidence of depression in peritoneal dialysis population is 50%.[491011] Looking at various demographic variables such as age, transplantation, education, Evans et al. had showed that Health Related Quality of Life (HRQoL) of ESRD patients were low and was associated with disturbance and quality of sleep. In a report of Italian study of Sf-36 on dialysis patients, females showed lower scores due to the impact of ageing on physical activities.[12] Depression is the most common psychological disorder among patients with end stage renal disease and has been associated with increased mortality inpatients maintained on hemodialysis therapy in an Indian study comparing MHD and CAPD patients, quality of life score was better in CAPD than hemodialysis 52.27 and 74.59, respectively, but within different socioeconomic status.[13]
In the present study, HRQoL was determined by the level of depression and other factors such as age, sex, hemoglobin, BMI, frequency of dialysis, erythropoietin dosage, economic status, past history of diseases, and duration of dialysis was also considered. The following were looked by multivariate analysis. The vintage of dialysis was significantly associated with depression (P = 0.02). The mental health score is also associated with depression (P = 0.03).Other factors associated with depression are female gender, limitation in performing vigorous activities, and difficulty in carrying out daily activities. Comparable to this study, a study from Iran, also showed that mental health (P = 0.01), role limitation of work due to physical and mental function (P = 0.05) shows a significant correlation with depression.[14]
In India, government contributes only 0.9% of GDP to health care facilities and 4.3% is by the private sectors. In order to speculate the possible mechanisms of the negative impact of low income on the self-perceived health status, several explanations have been proposed, including differences in lifestyle, exposure to different stresses, and differences in available supportive resources.[14]
Not only the negative impact of low income on HRQoL was seen in our renal transplant recipients, but also the anxiety level was higher in this population. It was shown that low-income renal transplant recipients were more likely to experience allograft failure after 1 and 5 years of the graft function than patients with adequate income due to their psychological stress and anxiety.[14] In India, 3.25 renal transplantations are done per million population from live and deceased donors; it is grossly inadequate where the incidence of ESRD is 150/million population and majority have to stay alive in MHD therapy.[15] Despite support by the government, it is believed that economic status still plays a dominant role in access to health care and quality of care in some countries.[16]
Government's support for maintenance hemodialysis is grossly inadequate in India. Medical insurance coverage is available only to a small minority for renal replacement therapy. The most reported literature concludes that it is the low income that causes ill health. Whatever the direction is, the important point is that the link between poor health and poverty should be broken by health policy makers.[17] The prevalence of poor sleep in maintenance hemodialysis patients was 71% and low HRQoL in all domains of SF-36.Correction of anemia with erythropoietin reduces arousals from sleep and sleep fragmentation.[18]
In this study, patients receiving 10 000 units/week of erythropoietin therapy had higher hemoglobin level and have good quality of life scores.
The main limitation of this study is that this is a cross-sectional study. It was not possible to measure all variables that may affect the quality of life like alcohol, caffeine consumption, etc. The association of depression in BPL patients is significant in this study, which is one of the predominant indicators for predicting the mortality of ESRD patients. Private and public sector partnership should support RRT that can abrogate depression in these patients. As India has the second-largest GDP growth rate, policymakers should allocate more money for renal replacement therapy in dialysis patients. The MHD patients should not be stigmatized and those who are functionally active should be fruitfully employed to improve self-esteem and thereby depression.
Conclusion
The factors that were identified in this study that influence depression such as poverty status, increasing age, vintage and frequency of dialysis, anemia treatment with erythropoietin dosage should be addressed and treated accordingly to improve the quality of life in maintenance hemodialysis patients. Improving self-esteem with fruitful employment opportunities, concerted rehabilitation by professionals, and easing of economic burden by private–public partnership is an achievable and often under a recognized goal.
Source of Support: Nil
Conflict of Interest: None declared.
References
- The challenges of renal replacement therapy in Asia. Nat Clin Pract Nephrol. 2008;4:643.
- [Google Scholar]
- Analysis of depression and morbidity index and its effect on outcome among chronic peritoneal dialysis patients. Indian J Perit Dial. 2009;17:72-5.
- [Google Scholar]
- The association of Sf-36 quality of life scale with patients on mortality. Fresenius Med Care. 2000;35:293-300.
- [Google Scholar]
- Psychological adaptations and quality of life of the patient with ESRD. Vol 15. Oxford: Oxford University Press; 1999. p. :1911-3.
- Multiple measurements of depression predict mortality in a longitudinal study of chronic hemodialysis outpatients. Kidney Int. 2000;57:2093-8.
- [Google Scholar]
- Dialysis outcomes and hospitalization among hemodialysis patients in the United States and Europe. Kidney Int. 2002;62:2238-45.
- [Google Scholar]
- Health-related quality of life in dialysis patients. A report from an Italian study using the SF-36 Health Survey. DIA-QOL Group. Nephrol Dial Transplant. 1999;14:1503-10.
- [Google Scholar]
- Is the SF-36 suitable for assessing health status of older stroke patients? Age Ageing. 1998;27:19-22.
- [Google Scholar]
- Depression and its associations with peritonitis in long-term peritoneal dialysis patients. Am J Kidney Dis. 2003;42:350-4.
- [Google Scholar]
- Diagnosis of depression in patients with end-stage renal disease. Comparative analysis. Am J Med. 1985;79:160-6.
- [Google Scholar]
- Depression in chronic dialysis patients : Assessment and treatment. Nephrol Dial Transplant. 2000;15:1911-3.
- [Google Scholar]
- Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J Am Soc Nephrol. 2001;12:2797-806.
- [Google Scholar]
- Quality of life and cost utility: Comparison of Hemodialysis versus Peritonial dialysis in India. 4th Congress of International Society of Hemodialysis. 2011;50 D43
- [Google Scholar]
- Evolution of renal transplantation in India over the last four decades. Clinical Kidney Journal. 2010;3:203-7.
- [Google Scholar]
- Socioeconomic links to health-related quality of life, anxiety, and depression in kidney transplant recipients. Iran J Kidney Dis. 2009;3:40-4.
- [Google Scholar]
- Quality of sleep and health-related quality of life in hemodialysis patients. Nephrol Dial Transplant. 2009;18:126-32.
- [Google Scholar]




