

Translate this page into:
Succesfully treated Curvularia lunata peritonitis in a peritoneal dialysis patient
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Fungal peritonitis is a rare but serious complication of peritoneal dialysis (PD) and is associated with significant mortality. It accounts for approximately 2–7% of PD-related peritonitis, which is difficult to clear, can result in catheter loss, and can frequently lead to conversion to hemodialysis. Fungal peritonitis usually follows the episode of bacterial peritonitis treated with antibiotics. The most common causative agent for fungal peritonitis is Candida species.[1] But these days several other yeasts and filamentous fungi are increasingly being reported. We report herein a patient of CAPD peritonitis with Curvularia lunata and its management.
A 55-year-old housewife, on CAPD for end stage renal disease (ESRD-nondiabetic) for 18 months presented with fever of 3 days duration with diffuse abdominal pain and cloudy bag. There was no history of cough, dysuria, and diarrhea. CAPD fluid microscopy showed neutrophilic leukocytosis (12 500 cells/mm3). Gram stain showed plenty of pus cells and occasional gram negative bacilli. Enterobacter aerogenes was grown in culture, sensitive to amikacin, cefoperazone, sulbactam, ceftazidime, ciprofloxacin, gentamicin, imipenem, piperacillin, tazobactam. Ziehl–Neelson staining for acid fast bacilli was negative and KOH mount did not reveal any fungal elements. Patient recovered with intraperitoneal ceftazidime, cefazolin, amikacin, and oral fluconozale tablets for 3 weeks. Almost at the completion of treatment of peritonitis patient presented with difficulty in drainage of CAPD fluid, the presence of lack colored small fragments in CAPD catheter, transfer set and drain bag since 3 days. There was no fever and abdominal pain.
The microbiological evaluations of the CAPD fluid and black fragments revealed dematiaceous septate fungal hyphae in KOH mount [Figure 1]. Gram stain showed pus cells but no organism, culture was sterile after 48 h of aerobic incubation. Fungus culture on Saboraud's dextrose agar (SDA) was positive within 48 h. The colonies on SDA were woolly, white to pinkish gray colored initially which turned olive brown and black later. The colonies were dark brown to black from the reverse. Lactophenol cotton blue mount of the colonies on SDA showed septate, brown hyphae, brown conidiophores, and conidia. Conidiophores showed sympodial geniculate arrangement. The conidia were pyriform, brown, and multiseptate. There were three transverse septa in each conidium. Based on the growth characteristics on SDA and lactophenol cotton blue mount of the growth the isolate was identified as C. lunata species [Figure 2].
Though commonly isolated as contaminants, Curvularia sp are capable of causing infections in humans as well as animals. It is a dematiaceous fungus, present in the environment all around the world mainly tropical and subtropical regions. The genus Curvularia comprises several species like C. lunata, Curvularia pallescens, Curvularia senegalensis, Curvularia brachyspora, Curvularia clavata, Curvularia geniculata, and Curvularia verruculosa. Of these C. lunata is most commonly reported from various infections in humans. Curvularia sp. are known to cause several types of infection in immunocompetent as well as immunocompromised hosts.[2]
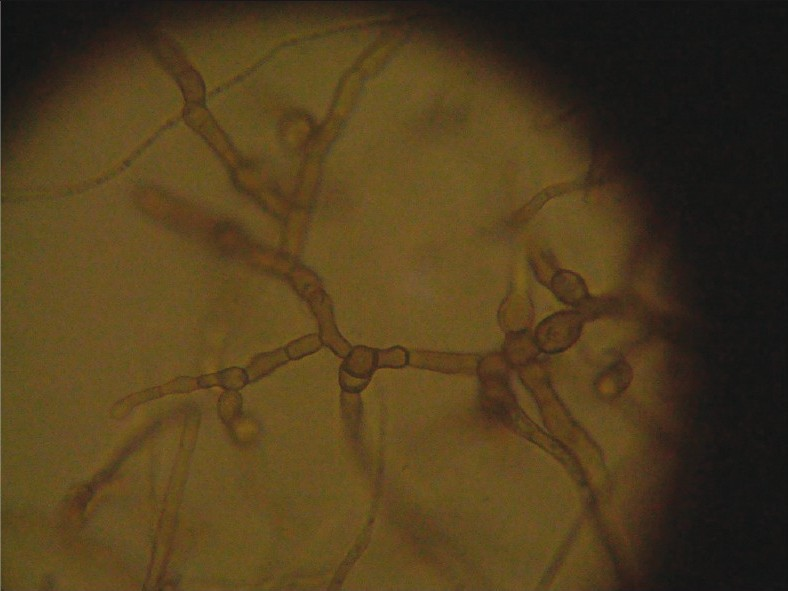
- KOH mount of the peritoneal fluid showing dematiaceous septate hyphae

- Lactophenol cotton Blue Mount of the colonies grown on Sabouraud's Dextrose agar showing septate, brown hyphae, brown conidiophores, and conidia. Conidiophores showed sympodial geniculate arrangement. The conidia were pyriform, brown, and multiple
In recent reports on patients of curvularia infection, it was observed that there can be three forms of presentation: (1) catheter obstruction without peritonitis, (2) catheter obstruction with peritonitis, and (3) only peritonitis.[3]
Treatment modalities for fungal infections include combination of amphotericin B and flucytosine for initial therapy. Amphotericin B, itraconazole, and terbinafine have so far been used to treat Curvularia infections. Voriconazole or posaconazole can be used as alternate to amphotericin B that causes chemical peritonitis.[4] According to an earlier report fluconazole prophylaxis was significantly effective in preventing secondary fungal infection in patients who were treated for bacterial peritonitis in CAPD.[5] However, we encountered fungal peritonitis due to curvularia despite fluconazole prophylaxis during treatment of bacterial peritonitis in our patient.
Patient was shifted to maintenance hemodialysis after catheter removal, and was treated with Tab. Voriconazole 400 mg B.D loading dose and 200 mg B.D maintenance dose for 3 weeks. At present patient is asymptomatic on regular follow-up.
The points of interest in our presentation are: development of a rare entity C. lunata-related peritonitis probably secondary to earlier antibiotic usage and its response to voriconazole.
References
- Clinical features of and risk factors for fungal peritonitis in peritoneal dialysis patients. J Formos Med Assoc. 2000;99:544-8.
- [Google Scholar]
- Human Curvularia infections. Report of five cases and review of the literature. Diagn Microbiol Infect Dis. 1987;6:27-39.
- [Google Scholar]
- Black specks in dialysis fluid: An unusual case of peritonitis in a pediatric patient on peritoneal dialysis. Dial Transplant. 2010;39:445-8.
- [Google Scholar]
- Peritoneal dialysis –Related infections recommendations: 2010 update. Perit Dial Int. 2010;30:393-423.
- [Google Scholar]
- Ten years without fungal peritonitis: a single center's experience. Perit Dial Int. 2007;27:460-3.
- [Google Scholar]




