

Translate this page into:
Emphysematous infections of the urinary tract: A radiological perspective
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Emphysematous pyelonephritis (EPN), first described in 1898, is a life-threatening necrotizing infection of the upper urinary tract characterized by gas formation within or surrounding the kidneys. Early diagnosis and immediate management are crucial for a favorable clinical outcome. Predisposing factors are diabetes mellitus, low immune status, urinary tract obstruction due to uroliths, neoplasm or sloughed papilla, end-stage renal disease, chronic alcoholics and post renal transplant. Diabetes is the most common culprit with women being affected at least twice as often as men, with the female-to-male ratio reported to be as high as 6:1.[1–3] The pathogenesis of EPN in diabetics relates to high levels of tissue glucose which provide a favorable environment for acidic fermentation of gas-forming microbial organisms, impaired tissue perfusion and a defective immune response. Organisms causing EPN are E. coli, Klebsiella, Proteusand Pseudomonas.
Computed tomography (CT) is the imaging modality of choice. Conventional radiography demonstrates mottled gas in the renal fossa and obscuration of psoas shadows [Figure 1]. On ultrasound, echogenic foci of gas with reverberation artifacts are seen. Renal calculi, artifacts, and bowel gas may also be erroneously diagnosed as EPN on ultrasound. Unenhanced CT is generally sufficient and considered the most sensitive and specific modality.Contrast-enhanced CT done at approximately 50-90 secs (nephrographic phase) after injection provides additional detailed information regarding anatomy, extent of spread of infection, pattern of renal enhancement, complications like tissue necrosis, abscess formation and if required delayed phase at 3-5 mins (excretory phase) imaging may be done only if urinary tract obstruction is suspected [Figures 2 and 3].
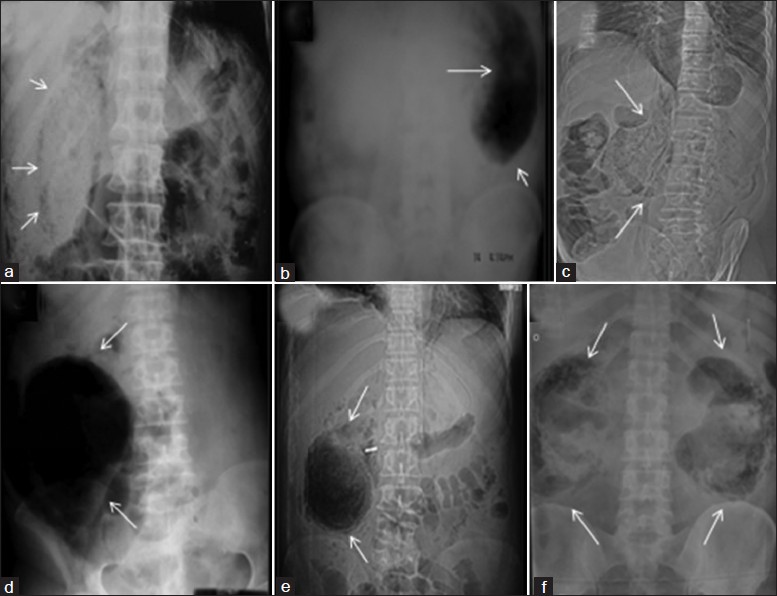
- Plain X-ray KUB showing spectrum of EPN in various patients (a) air (arrows) in the right perirenal space outlining the right kidney, (b) left renal fossa completely replaced by air (arrows), (c) mottled air lucencies (arrows) in right renal fossa obscuring the right psoas shadow, (d) right renal fossa completely replaced by air (arrows) obscuring psoas shadow, (e) mottled air lucencies in right renal fossa (arrows) with Ryle's tube in situ, (f) mottled air lucencies (arrows) in bilateral renal fossa

- Axial contrast-enhanced CT scan showing non enhancement of right renal parenchyma and air (arrows) in right renal and perirenal space suggestive of Type I EPN

- Axial non-contrast CT scan showing bilateral Type II EPN with air (arrows) in the pelvicalyceal system and pyonephrosis in left kidney with mild left perinephric stranding
The differential diagnosis of gas in the renal parenchyma includes other than EPN are focal renal abscess, accidental or iatrogenic trauma to the kidney or bladder (e.g., from surgery, biopsy, urinary bladder catheterization, nephrostomy tube placement), and enterorenal fistula.
Two classification systems have been used for EPN for predicting prognosis. Wan et al. classified EPN into two types. Type 1 EPN is acutely more fulminant, with streaky or mottled gas pattern and no adjacent fluid collections. Type 2 EPN has a lower mortality rate than type 1 EPN (18% vs 69%, respectively) and shows a bubbly gas pattern in the pelvicalyceal system and fluid either in the kidney or surrounding the kidney.
Another classification system [Table 1] proposed by Huang and Tseng[4] focuses on theclinicoradiological classification, management and prognosis.

Emphysematous pyelitis, a less aggressive form of infection of the upper urinary tract is diagnosed when gas is localized to the renal collecting system. It is more common in females with diabetes and urinary tract obstruction and has a favourable outcome. Conventional radiography demonstrates gas in the renal excretory system. On ultrasound, nondependenthigh-amplitude flat echoes within the pelvicalyceal system areseen. CT is the modality of choice and reveals gasbubbles or gas-fluid levels localized within the pelvicaliceal system [Figure 4] sparing the renal parenchyma.[5] Reflux of air during instrumentation and the presence of an ilealureterosigmoidostomy can also result in air within the renal excretory system. Management includes intravenous antibioticsand drainage of collections.

- Axial non-contrast CT scan showing air (arrows) in bilateral pelvicalyceal system suggestive of bilateral emphysematous pyelitis. Mild perinephric stranding is seen bilaterally with subcutaneous edema and stranding in right abdominal wall muscles (arrowhead)
Emphysematous cystitis, a rare fulminant disease of the urinary bladder is seen in patients with diabetes mellitus, neurogenic bladder, obstructive uropathy and recurrent infections. Conventional radiography reveals characteristic curvilinear or mottled lucencies in the pelvis, air-fluid level that changes with patient position and a cobblestone or “beaded neck-lace” appearance representing air.[2] On ultrasound, bladder wall thickening, echoes with posterior dirty acoustic shadowing is seen. CT is highly sensitive showing intraluminal/intramural gas [Figure 5]. Differnentials include gas due to enteric fistula from adjacent malignancy or inflammation. CT cystography is superior in identifying a vesicocolic fistula.

- Axial contrast-enhanced CT demonstrating emphysematous cystitis showing air (arrows) within the wall of urinary bladder and mild free fluid in pelvis
Treatment involves broad-spectrum antibiotics, hyperglycemic control, and adequate urine drainage with correction of possible bladder outlet obstruction when present.[2]
Dr. BB Thukral and Dr. Aliza Mittal for support and guidance
Source of Support: Nil
Conflict of Interest: None declared.
References
- Presentation and outcome of emphysematous renal tract disease in patients with diabetes mellitus. UrolInt. 2007;78:13-22.
- [Google Scholar]
- Emphysematous infections of theabdomen and pelvis: A pictorial review. Radiographics. 2002;22:543-61.
- [Google Scholar]
- AJR Teaching File: Diabetic patient presenting with right flank pain and fever. AJRAm J Roentgenol. 2010;194:WS31-3.
- [Google Scholar]
- Emphysematous pyelonephritis: Clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med. 2000;160:797-805.
- [Google Scholar]




