

Translate this page into:
A case of Down syndrome with a posterior urethral valve
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
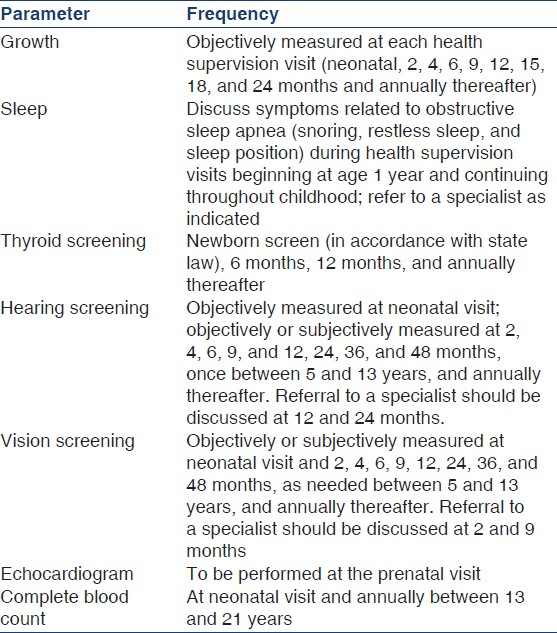
Down syndrome is characterized by multiple congenital abnormalities, particularly cardiac defects (26-50%), eye disease (60%), hearing loss (75%), obstructive sleep apnea (50-75%), gastrointestinal atresia (12%), and thyroid disease (15%). The committee on genetics of the American Academy of Pediatrics (AAP) has provided recommendations to assist pediatricians in care of children with Down syndrome. These recommendations are summarized in Table 1. Renal function tests and a routine ultrasonography of the abdomen do not feature in these recommendations. Both upper and lower urinary tract anomalies like hypoplasia of kidney, glomerular microcysts, dysplastic kidney, and obstructive uropathy have been described in Down syndrome. Posterior urethral valve (PUV) is rarely associated with Down syndrome. Renal anomalies may thus be underreported in Down syndrome.
A 6-month-old male child presented with complaints of decreased urine output for the last 2-3 days. On reviewing of history it was learnt that there was difficulty in passing urine since birth. The child was the 8th according to birth order. There was a history of three sibling deaths at 9 months, 1 month, and 6 years of age respectively due to unknown causes. On examination, signs of dysmorphism like large tongue, slanted eyes, epicanthic folds, simian crease, short, and broad hand with short middle phalanx of fifth finger were noted. Cardiovascular examination revealed no congenital heart disease. Abdominal examination showed bilateral renal masses. Urinary bladder was palpable up to the level of umbilicus.
Investigations revealed hemoglobin of 8.5 g/dl, TLC-14,600/μl, and platelet count 196,000/μl. Urin-alysis was normal and urine cultures were sterile. Renal functions were deranged with blood urea 189 mg/dl and creatinine 4.8 mg/dl. Serum electrolytes assay revealed serum sodium 126 meq/l, potassium 7.1 meq/l, and ionic calcium 4.6 mg/dl. There was no acidosis. Ultrasonography of abdomen revealed gross hydronephrosis with right kidney measuring 5.9 × 3.3 cm and left kidney measuring 6.2 × 3.9 cm; bilateral ureters were dilated and tortuous in entire length. Micturating cystourthrogram showed irregular outline of the bladder wall with evidence of outpouching suggestive of diverticulae/sacculation, posterior urethra appear dilated with normal distal urethra, and bilateral ureters were grossly dilated with grade V vesicoureteric reflux with grade III/ IV hydronephrosis. Karyotyping revealed 47 XY+21 chromosome; consistent with the diagnosis of Down syndrome. After decompressing the bladder with an indwelling catheter, the child's serum potassium and kidney functions improved. The case was referred to a pediatric surgeon, and according to their advice, was referred to the pediatric surgery department for the definitive procedure.
In 1960, Berg et al. first noted coincidence of renal anomalies and Down syndrome.[1] They reported that 5 of 141 Down syndrome autopsy cases (3.5%) had renal malformations. Four of these patients had renal agenesis or hypoplasia, and one had a horseshoe kidney. In a more current autopsy/necropsy study, Ariel et al. examined 124 cases of Down syndrome for urinary system abnormalities like renal hypoplasia, glomerular microcysts, cystic dysplasia, and simple renal cysts.[2]
Down syndrome associated with PUV with visicoureteric reflux is not commonly reported. Ahmed detailed four cases of Down syndrome associated with reflux.[3] Two of the four children required nephrectomy for advanced reflux nephropathy. The other two children underwent ureteral reimplantation, but surgery was unsuccessful. Kupferman et al.[4] reported three patients with Down syndrome and posterior urethral valves. This study was followed by Bielek et al.,[5] who reviewed experience at their institution. They found that of 48 cases of PUV, 2 (4.17%) had trisomy 21. Recently, Kim et al.[6] reported a case of posterior urethral valve, hydronephrosis, and hydrothorax associated with Down syndrome diagnosed antenatally and treated it successfully with intrauterine shunt. In 2002, Michael et al. reported a case of a 19-year-old male presented with renal failure due to posterior urethral valve.[7]
In conclusion, renal anomalies are probably under reported in Down syndrome. PUV is a treatable cause of renal failure. Therefore, we suggest that screening for renal anomalies should be a part of routine evaluation in a child with Down syndrome.
References
- The urinary system in Down syndrome: A study of 124 autopsy cases. Pediatr Pathol. 1991;11:879-88.
- [Google Scholar]
- Vesicoureteric reflux in Down's syndrome: Poor prognosis. Aust N Z J Surg. 1990;60:113-6.
- [Google Scholar]
- Posterior urethral valves in patients with Down syndrome. Pediatr Nephrol. 1996;10:143-6.
- [Google Scholar]
- A rare case of posterior urethral valve and pleural effusion in Down syndrome with successful intrauterine shunt. Fetal Diagn Ther. 2008;24:372-5.
- [Google Scholar]




