

Translate this page into:
Post-infectious glomerulonephritis following infective endocarditis: Amenable to immunosuppression
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Glomerulonephritis develops in about 20% patients with infective endocarditis (IE), but is mostly asymptomatic. Heavy proteinuria or derangement of kidney functions is uncommon. We report here a child with IE and proliferative glomerulonephritis who manifested as significant proteinuria that recovered on treatment with immunosupressants.
Keywords
Infective endocarditis
post-infectious glomerulonephritis
proliferative glomerulonephritis

Introduction
Infective endocarditis (IE) is often a complication of congenital or rheumatic heart disease in children. Despite appropriate antibiotics, IE carries a high mortality. The infection-related complications of IE include myocardial abscess, meningitis, osteomyelitis, renal abscess and purulent pericarditis. The embolic complications are manifested by stroke, sudden-onset blindness and pulmonary thromboembolism. Renal involvement occurs in about 25% of the patients with IE, but most are asymptomatic.[1] The most common pathological renal lesions described are renal infarcts, glomerulonephritis and interstitial nephritis.[2] While most of these complications improve upon use of appropriate anti-microbial agents, rarely, immunosuppressants have been used for the treatment of glomerulonephritis not responding to mentioned therapy.[3] We report here a child with post-IE glomerulonephritis that resolved on use of immunosupression.
Case Report
An 11-year-old boy, a known case of acyanotic heart disease since infancy, was admitted with high-grade fever for 15 days. He had cough, respiratory distress, and chest pain for 1 day. On examination, he was conscious but sick looking and had pallor. His pulse rate was 140/min, with all peripheral pulses well palpable. His respiratory rate was 76/min and he had subcostal and intercostal recessions. The blood pressure was 102/60 mmHg. On examination of the chest, the child had bilateral fine crepts. The cardiovascular examination was suggestive of cardiomegaly. A grade 3/6 systolic murmur was heard all along the left sternal border. The second heart sound was loud and palpable. The liver was palpable 5.0 cm below the costal margin and the spleen was palpable 3 cm below the costal margin. A provisional diagnosis of congestive heart failure with a possibility of IE was made.
The investigations revealed a hemoglobin concentration of 5.6 g/dL with a microcytic and hypochromic picture. The total leucocyte count was 18,650 (polymorphs 70, lymphocytes 25, eosinophils 2, monocytes 2) and the platelet count was 102,000/mm3. All the three blood cultures sent were sterile. A chest X-ray showed cardiomegaly with congested lung fields. An urgent echocardiogram revealed an atrial septal defect (7 mm) and a restrictive perimembranous ventricular septal defect (5 mm) with multiple vegetations in the right ventricle at the site of impingement of jet and near the ventricular septal defect. A urine examination revealed 2+ proteinuria and 15-20 RBCs/hpf (40% dysmorphic). The kidney function tests showed urea of 64 mg/dl and creatinine of 0.8 mg/dl. A fundus examination revealed bilateral Roth’s spots. A diagnosis of IE with congestive heart failure was made. The child was started on furosemide and intravenous ceftriaxone, vancomycin, and gentamicin. The child received packed cell transfusion. After 5 days his renal functions worsened (urea 58 mg/dl and creatinine 1.7 mg/dl). The antibiotics were changed to piperacillin-tazobactam, teicoplanin and gentamicin in view of renal dysfunction and persistence of fever. Subsequently, the antibiotics were upgraded to meropenem and teicoplanin in view of non-response. The child received antibiotics for a total duration of 6 weeks. The fever subsided but the patient developed periorbital puffiness and his proteinuria increased to 3+ and renal functions continued to be deranged (urea 114 mg/dl, creatinine 1.2 mg/dl). The urinalysis after 6 weeks of antibiotic therapy showed 2+ proteinuria, 18-20 RBC/hpf and 20-25 casts/hpf (both fine and course).
A renal biopsy done at this time showed moderate degree of chronic parenchymal damage in the form of tubular atrophy and interstitial fibrosis on Masson’s Trichrome stain [Figure 1a]. There were 19 glomeruli, of which four were globally sclerosed. The viable glomeruli showed increase in mesangial matrix and cellularity with focal endocapillary proliferation [Figure 1c and d]. Two glomeruli showed partial cellular to fibrocellular crescents [Figure 1b-d]. The basement membrane was unremarkable on silver methenamine stain.
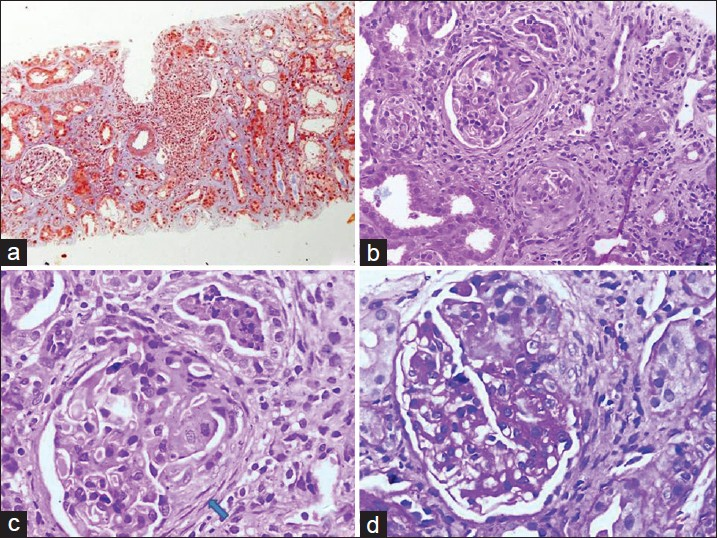
- Light microscopy photomicrographs. (a) Low power view photomicrographs - Masson’s Trichrome stain displaying chronic parenchymal damage; dense chronic inflammatory cell infiltrate seen in the interstitium (× 100). (b and c) H and E stained photomicrographs displaying partial fibrocellular crescents (arrow) and mild increase in mesangial matrix and cellularity (× 200 and × 400 respectively). (d) periodic acid - Schiff stained photomicrographs at high power (× 400) displaying a partial cellular crescent and mild increase in mesangial matrix and cellularity
Immunofluorescence showed fine granular deposition of C3, C1q and IgM in the glomerular capillary walls and mesangium [Figure 2]. Two crescents were positive for fibrinogen stain. A diagnosis of a receding phase of immune complex-mediated proliferative glomerulonephritis with crescents was made.
The anti-nuclear antibody was negative and antistreptolysin (ASLO) titers were normal, and C3 complement levels were 117 mg/dl. The serology for hepatitis B surface antigen and anti-HCV were negative. The child continued to have protienuria and also developed edema, while his heart failure was controlled. His total serum proteins were 6.0 g/dl and he had a serum albumin level of 2.8 g/dl. His cholesterol was 190 mg/dl. In view of persistent proteinuria, the child was started on oral prednisolone 2 mg/kg/day for 4 weeks. The child continued to have proteinuria and edema persisted. In view of a proliferative glomerulonephritis on renal biopsy, oral cyclophosphamide was added in doses of 2 mg/kg/day for 8 weeks with alternate-day steroids. At the end of treatment, the child became edema free. His urine protein was negative and his kidney functions had normalized (urea 27 mg/dl and creatinine 0.8 mg/dl). The child has been on follow-up for the last 1.5 years, and has continued to be well. He is off all medications at present.

- Immunofluorescence photomicrographs C3 and IgM stained glomeruli displaying fine granular deposition of immune complexes in the peripheral capillary walls and mesangium (× 400)
Discussion
Systemic embolization as a complication of endocarditis was first described by Virchow in 1858.[4] Since then, three different forms of renal diseases have been identified with IE. These are a post-infectious immune complex-mediated glomerulonephritis, an embolic disease or a drug-induced acute interstitial nephritis. The glomerular lesions are focal or diffuse proliferative, and are assumed to be immune complex mediated. Drug-induced acute interstitial nephritis is primarily related to use of antibiotics like aminoglycosides, vancomycin and amphotericin-B for the treatment of IE. The most common indications for renal biopsy in a child with IE are deranged renal function, presence of significant proteinuria or rapidly progressive renal failure.
The incidence of complications related to IE have decreased since the use of better antibiotics. Most infective and non-infective complications of IE resolve on treatment with appropriate antibiotics. However, there have been instances where, despite the use of these drugs, the renal lesions have not improved. We came across few reports that showed corticosteroids to be useful for IE-induced glomerulonephritis.[356] Rarely, oral cyclophosphamide has also been used for amelioration of symptoms. Non-response to antibiotics in our patient led to the use of corticosteroids and cyclophosphamide in view of proliferative lesions on renal biopsy. Fortunately, he responded to therapy and his renal parameters became normal.
We conclude that proliferative lesions on renal biopsy in a patient with IE are ameliorable to immunosuprressants. While all efforts should be made to treat the complications with antibiotics, a non-response may require the use of either steroids alone or in combination with oral cyclophosphamide for the treatment of proliferative lesions on biopsy.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Use of corticosteroids in glomerulonephritis related to infective endocarditis: Three cases and review. Clin Infect Dis. 1999;28:1057-61.
- [Google Scholar]
- Cellular Pathology. New York: Dover Publications; 1971. p. :243-4.
- Renal pathological findings in infective endocarditis. Nephrol Dial Transplant. 2000;15:1782-7.
- [Google Scholar]
- Crescentic glomerulonephritis in a child with infective endocarditis. Pediatr Nephrol. 2006;21:867-9.
- [Google Scholar]




