

Translate this page into:
Extended spectrum beta lactamase peritonitis: Our experience
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
We read with interest the article of Dr. Sinha and Coll[1] on extended spectrum beta-lactamase (ESBL) peritonitis in patient on chronic peritoneal dialysis (PD). The guidelines of International Society for PD[2] state that the selection of empiric antibiotics must cover all serious pathogens that are likely to be present, through a first-generation cephalosporin, such as cefazolin or cephalothin, with a second drug for broader Gram-negative coverage (including coverage for Pseudomonas) such as aminoglycoside, ceftazidime, cefepime, or carbapenem.
The guidelines of Italian Society of Nephrology state that intra-peritoneal (IP) administration of antibiotic agents is the most effective treatment of PD peritonitis; intermittent administration may be preferred to continuous administration of antibiotic agents in PD peritonitis.[3] We routinely, apply these guidelines in our clinical practice. We would like to report our similar experience: A 65-year-old Caucasian patient, suffering from autosomal dominant polycystic kidney disease, on chronic PD, was admitted to hospital for signs and symptoms of peritonitis (fever, abdominal pain, cloudy PD fluid effluent, a cell count of 9950/ml). He was started on IP cefazolin and tobramicine and IV ciprofloxacin, but in the next 72 h he worsened vomiting and abdominal pain. Abdominal CT scan [Figure 1] showed the presence in the bowels of significant fluid with intense gaseous component. The PD fluid culture was confirmed to be ESBL secreting Pseudomonas aeruginosa. Due to the severe clinical status, not having yet of susceptibility, we changed the empiric therapy starting intravenous meropenem 500 mg every 8 h a day. We observed a dramatic clinical improvement in the next 24 hours with disappearance of abdominal pain and vomiting and recovery of feeding. Having later known the result of the susceptibility pattern, positive for meropenem (minimum inhibitory concentration 0.25), we began IP therapy with this drug (500 mg/2 L). The antibiotic was continued for 2 weeks and a repeat PD fluid analysis showed a normal cell count and sterile culture.
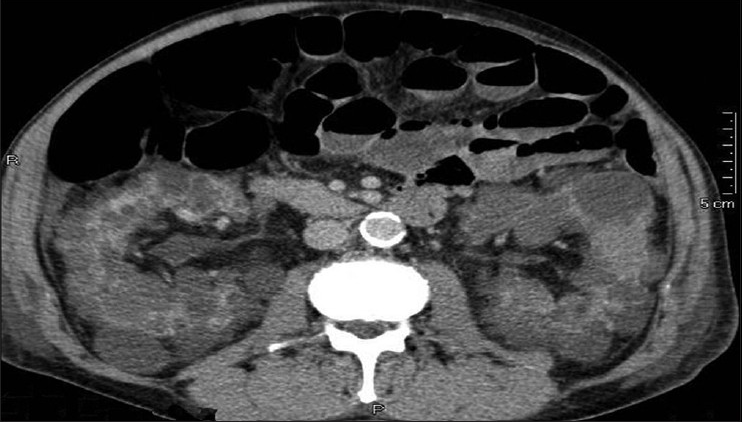
- Abdomen CT scan: Enlarged polycystic kidneys; presence in the bowel of significant fluid with intense gaseous component
Furthermore, in Italy, the menace of ESBL peritonitis is becoming increasingly common. We agree with the authors on the need for studies on the efficacy of meropenem in ESBL peritonitis and the best route of administration (IP or parenteral), as well as the need for a revision of the International Society for PD recommendations, incorporating suggestions for ESBL peritonitis.
References
- Extended spectrum beta lactamase peritonitis: Time for innovation? Indian J Nephrol. 2012;22:374-6.
- [Google Scholar]
- Peritoneal dialysis-related infections recommendations: 2010 update. Perit Dial Int. 2010;30:393-423.
- [Google Scholar]
- Treating peritonitis in peritoneal dialysis: Guideline from the Italian Society of Nephrology. G Ital Nefrol. 2007;24:149-64.
- [Google Scholar]




