

Translate this page into:
Chronic renal failure, hyperkalemia, and colonic ulcers
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 72-year-old male on regular hemodialysis presented to the emergency department with complaints of fatigue and watery diarrhea for 3 days. On examination, he was hypotensive. His medical history was significant for hypertension, chronic kidney disease, and was on regular hemodialysis. Investigations showed hyperkalemia (5.60 mEq/L). He was diagnosed to have acute on chronic kidney injury secondary to hypovolemia. He was treated with intravenous fluids, calcium resonium enema, and antihypertensives. Two days later, the patient had abdominal pain and bleeding per rectum. Diagnostic colonoscopy showed multiple colonic ulcers involving rectum to transverse colon [Figure 1]. The differential diagnoses included infectious and ischemic colitis. Colonic biopsies showed active colitis with mucosal ulceration. In addition, angulated purplish crystals with fish scale appearance were present on the mucosa, within the ulcer and inflammatory debris [Figures 2 and 3]. A diagnosis of calcium polystyrene sulfonate (CPS) induced colonic ulcers was made.
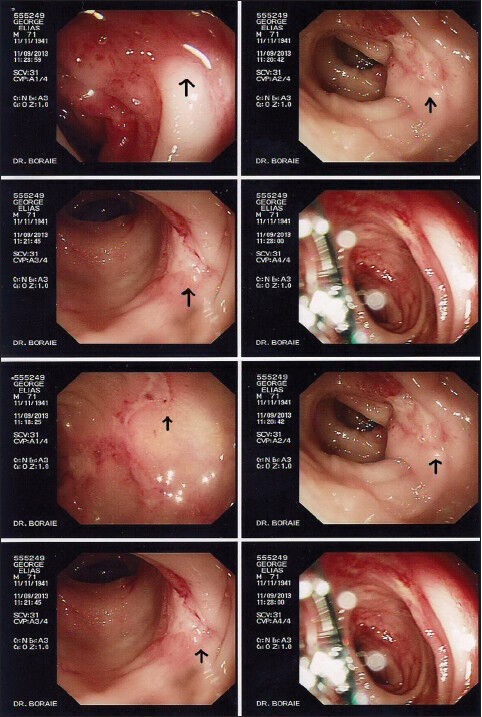
- Colonoscopy revealing mucosal ulcers (arrows) from rectum to transverse colon

- Purplish angulated crystals (arrows) within the colonic ulcers (H and E, ×400)
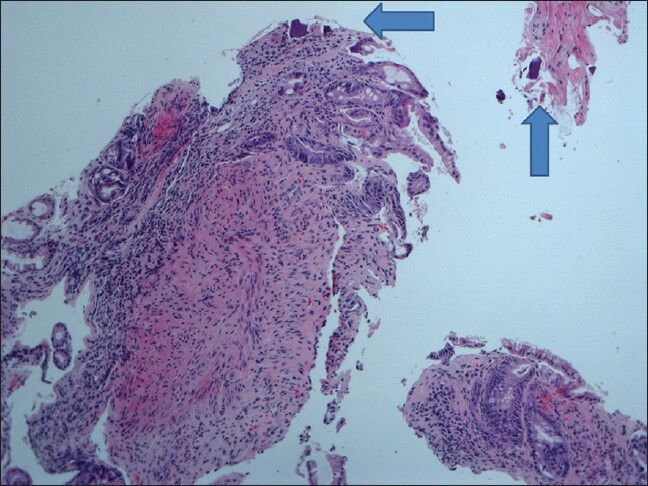
- Colonic mucosa with ulceration and purplish crystals (arrows) on the surface (H and E, ×200)
Sodium or calcium polystyrene sulfonate (Kayexalate/SPS or analog) is an ion-exchange resin commonly used to treat hyperkalemia. Colonic necrosis and perforation are rare, but may occur as severe complications associated with these drugs.[123] The actual incidence of gastrointestinal complications following SPS/CPS use is unknown, but is higher in patients with uremia and in posttransplant patients. Kayexalate induced colonic necrosis is usually diagnosed one to several days after administration, commonly occurs in the lower gastrointestinal tract but has been reported to occur in esophagus, stomach, and duodenum. The mechanism of the necrosis and perforation is unknown. Sorbitol is believed to be the toxic agent on the gastrointestinal mucosa.[2] However, use of kayexalate without sorbitol and CPS administered as suspension in distilled water has also been documented to cause the same complications. Hypovolemia, hyperreninemia, elevated prostaglandin production, and localized colonic mesenteric vasospasm are other possible explanations. Ischemic colitis, infectious colitis, and pseudomembranous colitis are the main differential diagnoses. The finding of characteristic angulated purplish crystals with fish scale appearance in the biopsy samples remain the main clue in the diagnosis of SPS/CPS induced colonic necrosis. These crystals are PAS positive and stain with acid-fast stains.[13] Histologically, SPS/CPS crystals should be differentiated from crystals of cholestyramine; the latter are more basophilic, rhomboid in shape, and opaque without a mosaic pattern. Clinicians need to be aware of these rare complications of potassium exchange resins.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Colonic necrosis and perforation due to calcium polystyrene sulfonate in a uremic patient: A case report. NDT Plus. 2011;4:402-3.
- [Google Scholar]
- Intestinal necrosis due to sodium polystyrene (Kayexalate) in sorbitol enemas: Clinical and experimental support for the hypothesis. Surgery. 1987;101:267-72.
- [Google Scholar]
- Colonic mucosal necrosis following administration of calcium polystyrene sulfonate (Kalimate) in a uremic patient. J Korean Med Sci. 2009;24:1207-11.
- [Google Scholar]




