

Translate this page into:
Urinary ascites after an alcohol binge: An uncommon treatable cause of acute kidney injury
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
A 38-year-old male presented after a binge of alcohol with acute onset, rapidly progressive distension of abdomen, hematuria, oligoanuria and dialysis dependent renal failure. Evaluation revealed ascitic fluid with high creatinine and computed tomography cystogram showed contrast leak into the peritoneum. Retrograde cystoscopy confirmed rupture of the bladder. He had prompt diuresis after indwelling Foley's catheter was placed. By 2 weeks, he had recovered renal function completely. A high index of suspicion can make an early diagnosis and avoid unnecessary investigations. The mechanism of spontaneous rupture of bladder after an alcohol binge is discussed.
Keywords
Acute kidney injury
alcohol
bladder rupture
urinary ascites

Introduction
Spontaneous rupture of the bladder is a potentially fatal condition.[1] It has been known to occur in a bladder weakened by disease process (neoplastic, neurogenic), radiotherapy for pelvic malignancies, postpartum state and after alcohol binge.[23] We present a case of spontaneous rupture of bladder after an alcohol binge, presenting as acute kidney injury (AKI). The diagnosis is not easy, but with a high index of suspicion, becomes obvious in most cases.[4] This patient was managed successfully by a conservative approach.
Case Report
The present case report is about a 38-year-old male patient, with no previously known comorbidities who had a binge of alcohol (approximately 300-400 ml rum) in the evening and fell asleep. He had acute onset of sudden severe epigastric pain at midnight. He gave history of reddish color urine initially which had cleared out over the next day. He was initially treated as a case of acute gastritis by a local practitioner with proton pump inhibitors, antacids and supportive care following which the pain subsided in 12 h. Over the next 3 days, he developed rapidly progressive distension of the abdomen and oliguria and became anuric by the 5th day. He was admitted to a peripheral hospital with these complaints. There was no history of fever, trauma, hematemesis, melena or jaundice. He had history of chronic alcohol intake of approximately 60-80 g ethanol/day for last 15 years. His family and past medical history were not contributory. He was found to have advanced azotemia with serum creatinine 6.4 mg/dl, although patient was not sick. He was transferred to the gastroenterology department of our hospital 1 week into his illness as suspected acute pancreatitis with AKI.
On examination, he was found to be in good general condition, having stable vital parameters with normal general physical examination. Systemic examination revealed gross ascites, no abdominal tenderness or guarding with no peripheral signs of liver cell failure or stigmata of cirrhosis.
Investigations revealed normal hemogram, normal liver function tests and normal amylase level. He had azotemia (blood urea nitrogen 46 mg/dl and serum creatinine 7.8 mg/dl) with normal electrolytes and serum protein levels. Ascitic fluid analysis revealed hemorrhagic, high serum ascites albumin gradient (3.9 g/dl) ascites with lymphocyte predominant cytology. His abdominal ultrasound Doppler showed normal liver, portal vein 7.8 mm, patent hepatic veins, normal pancreas, normal sized kidneys with preserved corticomedullary differentiation and gross ascites. Magnetic resonance imaging (MRI) abdomen revealed normal pancreas, ruling out acute pancreatitis and a mass in the urinary bladder. The radiologist suspected either a bladder malignancy or hematoma.
He was initially managed with two sessions of hemodialysis and supportive care. In view of the normal MRI findings, spontaneous rupture of the bladder was suspected. A repeat ascitic tap was done and an ascitic fluid creatinine of 33.7 mg/dl against a serum creatinine of 5.6 mg/dl clinched the diagnosis. Foley's catheter was passed and 6 l of urine was drained which led to the rapid disappearance of ascites. Computed tomography (CT) cystogram done subsequently, showed minimal leak of contrast into the peritoneal cavity [Figure 1]. Cystoscopy revealed a sealed perforation in the anterior bladder. He was managed conservatively by indwelling Foley's catheter for 2 weeks with rapid normalization of renal functions.
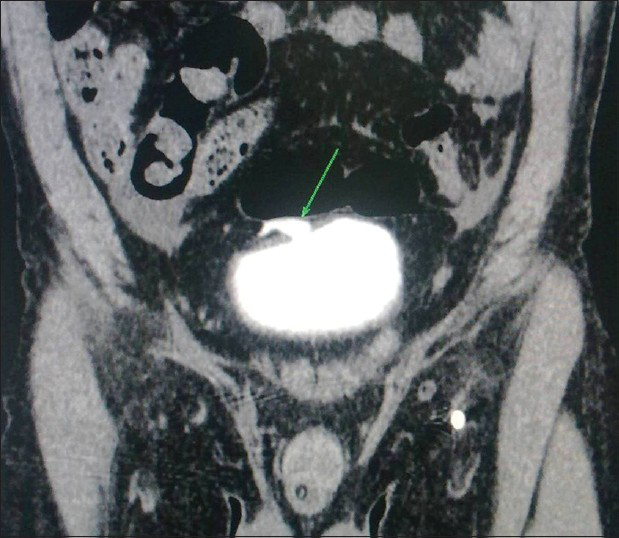
- Computed tomography cystogram showing intra-peritoneal leak of contrast
Discussion
Spontaneous or atraumatic rupture of the urinary bladder is an uncommon entity and if unrecognized, is associated with high morbidity and mortality.[4] Bladder rupture can be either intra-peritoneal or extra-peritoneal. Intra-peritoneal bladder rupture classically presents with a triad of abdominal pain, distension and urinary ascites. In the presence of known risk factors such as bladder neoplasms, radiotherapy for pelvic malignancies, neuropathic bladder, trauma, continuous bladder irrigation, postpartum state, bladder diverticulum or pelvic organ prolapse, the diagnosis is more straightforward.[3]
Intra-peritoneal leak of free urine results in lower abdominal pain, oliguria and laboratory features of AKI. The rapidly worsening renal failure is due to the process of “reverse auto dialysis” by the peritoneal membrane.[5] The peritoneum allows diffusion of urea and creatinine from the leaked urine into the blood and this leads to the subsequent rise in serum levels of urea and creatinine.
Our patient underwent unnecessary investigations initially with the mistaken diagnosis of acute pancreatitis. The most important factor in diagnosis is a high index of suspicion. A high ascitic fluid creatinine is suggestive;[6] CT cystogram and retrograde cystoscopy being confirmative. A bedside ultrasound of pelvis and bladder has been suggested by some as a sensitive method of suspecting bladder rupture, provided it is done by an experienced radiologist.[7] In the past, surgical repair of the bladder has been the mainstay of treatment; however conservative management was successful in our case.
In case of an alcohol binge, three factors contribute to the spontaneous rupture of the bladder.[7] Firstly, alcohol induced diuresis causes bladder distension and thinning of the bladder wall. Secondly, alcohol intoxication leads to altered sensorium and suppresses the urge of micturition. Thirdly, alcohol induced gastritis causes nausea and vomiting resulting in increased intra-abdominal pressure; thereby causing rupture of an over distended and thinned out bladder. This entity of spontaneous rupture of bladder should be kept in mind when an individual presents with pain abdomen, ascites and oliguric renal failure after an alcohol binge.
Source of Support: Nil
Conflict of Interest: None declared.
References
- An unusual cause of death: Spontaneous urinary bladder perforation. Am J Emerg Med. 2012;30:2081.
- [Google Scholar]
- Spontaneous bladder rupture in association with alcoholic binge: A case report and review of the literature. J Emerg Med. 2009;37:386-9.
- [Google Scholar]
- Spontaneous rupture of urinary bladder: A case report and review. Arch Ital Urol Androl. 2012;84:224-6.
- [Google Scholar]
- Idiopathic spontaneous bladder rupture in an intoxicated patient. Clin Nephrol. 2003;60:430-2.
- [Google Scholar]
- Bedside ultrasound diagnosis of atraumatic bladder rupture in an alcohol-intoxicated patient: A case report. Crit Ultrasound J. 2012;4:9.
- [Google Scholar]
- Spontaneous intraperitoneal rupture of a neurogenic bladder; the importance of ascitic fluid urea and electrolytes in diagnosis. Postgrad Med J. 1987;63:999-1000.
- [Google Scholar]




