

Translate this page into:
Renal tubular acidosis due to Sjogren's syndrome presenting as hypokalemic quadriparesis: A report of two cases
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Sjogren's syndrome is a chronic autoimmune disease with lymphocytic infiltration in the exocrine glands. Renal tubular acidosis (RTA) is a common extraglandular manifestation of this condition, which leads to hypokalemia. Although RTA with hypokalemia associated with Sjogren's syndrome has been reported earlier, hypokalemic quadriparesis as the initial manifestation of the disease is rare. We present two cases that presented as quadriparesis and were subsequently found to have Sjogren's syndrome.
A 25-year-old lady presented with sudden onset of weakness of all four limbs. Examination showed mild pallor and left parotid gland enlargement and flaccid quadriparesis with grade 1/5 power in all four limbs as well as neck muscle weakness. Deep tendon reflexes were absent, and sensations were intact. There was no bowel or bladder involvement. The differential diagnosis for acute flaccid paralysis such as Guillain-Barre syndrome, acute disseminated encephalomyelitis, and hypokalemic paralysis were considered. Results of relevant laboratory investigations are shown in Table 1. She had profound hypokalemia with normal anion gap metabolic acidosis, suggestive of distal RTA. Further evaluation revealed the presence of underlying Sjogren's syndrome.
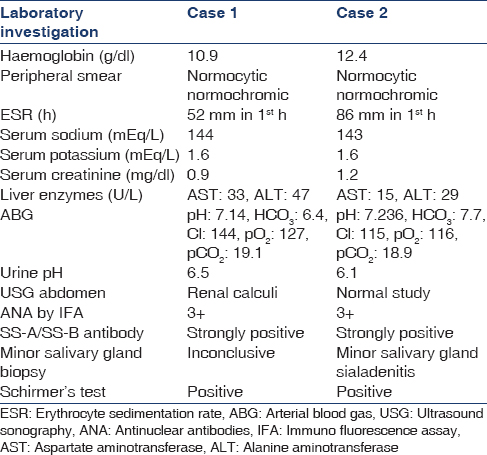
The second patient was a 45-year-old lady who presented with acute onset of quadriparesis of 2 days duration. She gave a history of similar episode 4 months earlier, which resolved with medication. General examination revealed pallor and glossitis. CNS examination revealed quadriparesis with grade 2/5 power in all four limbs, with normal sensations and preserved deep tendon reflexes. Her investigations are shown in Table 1. Since she was found to have severe hypokalemia with normal anion gap metabolic acidosis and alkaline urinary pH, a diagnosis of hypokalemic paralysis secondary to distal RTA was made. On questioning, she admitted to having symptoms of dry mouth and eye irritation for the past 6 months. However, there were no symptoms of other connective tissue disease. She was subsequently found to have Sjogren's syndrome.
Both the patients improved dramatically with intravenous potassium replacement.
Approximately one-third of patients with Sjogren's syndrome present with systemic manifestations.[1] The spectrum of the renal disease includes interstitial nephritis, which can manifest as distal RTA, proximal RTA, tubular proteinuria, nephrogenic diabetes insipidus, glomerular diseases, or renal failure. Hypokalemia is the most common electrolyte abnormality in patients with distal RTA.[2] However, a severe symptomatic decrease in serum potassium concentration has been described in a few cases only. In India, Rao et al. reported 31 cases of hypokalemic paralysis out of which, Sjogren's syndrome was found to be the etiology in three cases.[3] There have also been sporadic case reports.[45] Hypokalemic paralysis as the first manifestation of distal RTA due to Sjogren's syndrome is uncommon. It is worth noting that Sjogren's syndrome should be considered even in the absence of sicca symptoms as in ourfirst case.
Thus, patients presenting with hypokalemic paralysis due to RTA should be worked up for underlying primary diseases, such as Sjogren's syndrome, even in the absence of classic symptoms.
References
- American College of Rheumatology classification criteria for Sjögren's syndrome: A data-driven, expert consensus approach in the Sjögren's International Collaborative Clinical Alliance cohort. Arthritis Care Res (Hoboken). 2012;64:475-87.
- [Google Scholar]
- Aetiological, clinical and metabolic profile of hypokalaemic periodic paralysis in adults: A single-centre experience. Natl Med J India. 2006;19:246-9.
- [Google Scholar]




