

Translate this page into:
Dense renal medulla sign
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 50-year-old male, a known case of chronic liver disease, presented to us with abdominal distension for 2 days. Contrast-enhanced computed tomography (CT) scan revealed decompensated cirrhosis with portal hypertension. Clinically, the patient had features of dehydration. Plain CT sections revealed medullary regions of the kidney to be brighter than the cortex showing “dense renal medulla” sign (DRM) [Figure 1]. No calculus was seen in kidneys, ureter or in the urinary bladder. Urine examination revealed increased osmolality (970 mOsm/kg of water) and increased urine-specific gravity (1.037). The renal function tests were normal.
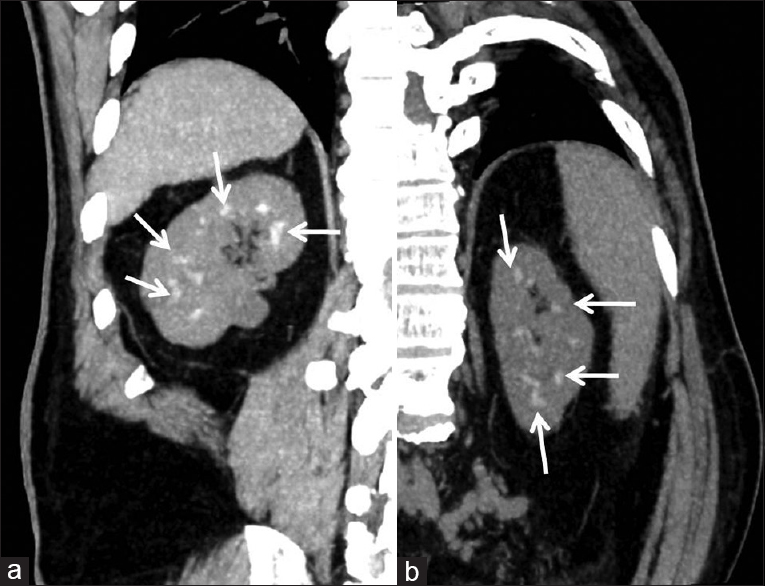
- (a) Coronal reformatted NCCT image showing hyperdense renal pyramids in right kidney (b) same patient oblique coronal reformatted image of left kidney in profile view showing hyperdense renal pyramids
Dense renal medulla is defined as increased attenuation of the medulla as compared to the renal cortex on plain CT scan.[1] It can be further divided into focal (confined to medullary tip) or global (involving entire medulla). Our case had global dense renal medullary involvement. DRM sign is also known as white pyramid sign or hyperdense renal pyramids sign. It is seen in conditions that increase urine osmolality (dehydration, hypernatremia, high-protein diet, glycosuria, adrenal insufficiency, and syndrome of inappropriate secretion of antidiuretic hormone), acute ureteric obstruction, high-dose antibiotic therapy due to antibiotic precipitation in collecting tubules, high caffeine intake, hyperparathyroidism, medullary sponge kidneys, medullary cystic disease, renal tuberculosis, sickle cell disease, renal papillary necrosis, and hyperuricemia.[2] Bilateral high-attenuation renal pyramids can occasionally be seen as an incidental finding. The presence of high-attenuation renal pyramids in only one kidney may suggest obstruction in the contralateral kidney.[3]
The most important differential diagnosis is medullary nephrocalcinosis. It is characterized by deposition of calcium salts in the medulla of the kidney. Serum and urinary calcium levels may be abnormal in these cases. Calcium salts which are deposited in medullary nephrocalcinosis mimic calcified concretions and reveal echogenic medullary pyramids on ultrasonography vis-á-vis DRM, which shows subtle hyperdensity as in this case. Ultrasonography is usually normal in cases of DRM. The disappearance of this hyperdensity following adequate hydration clinches the diagnosis. The index case had normal serum and urinary calcium levels, was dehydrated at the time of presentation, and renal ultrasound did not reveal echogenic medullary pyramids. Thus, dense renal pyramids in our case may be due to a combination of dehydration and high-protein diet advised in cirrhotic patients. We would like to conclude that dense renal pyramids should not be misinterpreted as medullary nephrocalcinosis by the radiologists and clinicians should be aware of this intriguing entity.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Effect of hydration status on renal medulla attenuation on unenhanced CT scans. AJR Am J Roentgenol. 1997;168:257-9.
- [Google Scholar]
- CT of renal densities caused by intravenous infusion of antibiotics. J Comput Assist Tomogr. 1995;19:228-31.
- [Google Scholar]
- Pearls and pitfalls in the diagnosis of ureterolithiasis with unenhanced helical CT. Radiographics. 2000;20:439-47.
- [Google Scholar]




