

Translate this page into:
Crossed fused renal ectopia with Wolffian duct anomaly
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
A 50-year-old man presented with lower abdominal pain since 6 months. Physical examination revealed a palpable lump of size 10 cm × 4 cm on the right lower quadrant. Transabdominal ultrasound showed two fused kidneys which had malrotated pelvicalyceal system forming an “S” shaped anomaly called sigmoid kidney, type of crossed fused renal ectopia [Figure 1]. A grossly dilated tortuous tubular structure representing a persistent ureteric bud was seen at the base of the urinary bladder. Transrectal ultrasonography showing the opening of the lower end of the tubular duct into the prostatic urethra was seen. Intravenous pyelography (IVP) and micturating cystourethrogram showed a single ureter on the right which drained both the crossed fused renal moieties. The tubular structure previously mentioned was nonopacified on IVP. On magnetic resonance imaging (coronal, sagittal, and axial views) studies, the blind ending ureteric duct showed hyperintense signal on T1 and T2 sequences but a relatively low signal intensity to that of the pelvicalyceal system of the crossed fused kidneys and was not suppressed on stir sequence [Figure 2]. The clinical symptoms were related to dilatation of the duct. The patient had no history of urinary or infertility complaints. The patient was suggested surgery, but he refused further investigations and treatment.
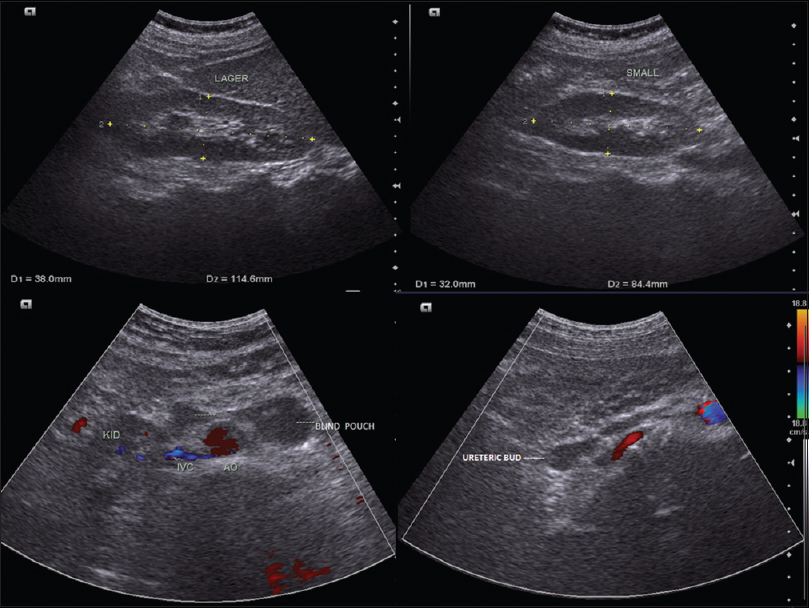
- Transabdominal ultrasound showed the presence of two kidneys fused at the pole on the right side and an empty left renal fossa. The fused kidneys had malrotated pelvicalyceal system forming an “S” shaped anomaly called sigmoid kidney. A grossly dilated tortuous tubular structure representing a persistent ureteric bud was seen at the base of the urinary bladder. It continued upward superiorly and on crossing midline ended in blind pouches near the aortocaval region, one of which was abutting the upper pole of the fused kidneys

- On magnetic resonance imaging (coronal, sagittal, and axial views) studies, the blind ending ureteric duct showed hyperintense signal on T1 and T2 sequences but a relatively low signal intensity to that of the pelvicalyceal system of the crossed fused kidneys and was not suppressed on stir sequence. The lower end of left ureteric duct is opening into the prostatic urethra
This is a case showcasing a rare association of sigmoid kidney on the right, absent seminal vesicle, and vas deferens on the left, along with obliteration of upper end of left ureteric bud. The sigmoid kidney is a subtype of crossed renal ectopia. There have been at least two cases of crossed renal ectopia with a ureterocele.[1] The crossed fused variety of renal fusion anomalies involves the two fused kidneys located on one side of the vertebral column. It has an incidence of 1:1300–1:7500,[2] lesser than that of horseshoe subtype. It has a male to female predominance of 3:2. It is more common to see the left kidney shift its location to the right and fuse with the right kidney.[3] Crossed fused ectopia has been further classified into several categories depending on what extent the fused kidneys are anatomically oriented.[4]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Cross ectopic multicystic dysplastic kidney with ureterocele in nonectopic site. Can Urol Assoc J. 2010;4:E61-3.
- [Google Scholar]
- Management of ureteral obstruction in crossed fused renal ectopia: A case report. Can Urol Assoc J. 2014;8:E752-4.
- [Google Scholar]
- Crossed-fused renal ectopia associated with inverted-Y ureteral duplication, ectopic ureter, and bicornuate uteruses. Urology. 2010;75:1175-7.
- [Google Scholar]




