

Translate this page into:
Spontaneous reno-colic fistula in an elderly patient
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 67-year-old woman was referred from a nursing home with fever and abdominal discomfort. She had multiple admissions for cerebral strokes in the past. There was no history of renal impairment or bowel complaints. Ultrasound showed marked left hydronephrosis with air foci within the renal pelvis, raising suspicion for emphysematous pyelonephritis. A contrast-enhanced computed tomography (CT) scan of abdomen and pelvis confirmed markedly dilated left pelvicalyceal system with a few air bubbles. There was no urinary calculus or dilatation of the ureter, suggesting long standing pelvi-ureteric junction (PUJ) obstruction. Interestingly, a track was noted between the left kidney and the splenic flexure [Figure 1a and b]. There was no abdominal lymphadenopathy, focal collection, peritonitis, or evidence of bowel inflammation or diverticular disease. There was no chest radiographic evidence of pulmonary tuberculosis. The sputum and urine tests for acid-fast bacilli were negative. No granulomas were identified in the liver or the spleen. Tumor markers were within normal limits. Percutaneous nephrostomy showed flow of contrast from left renal pelvis to splenic flexure [Figure 2]. A diagnosis of reno-colic fistula was made. Urine culture grew enterococci. Following the drainage and intravenous antibiotics, patient's general condition improved within 36h with resolution of symptoms. The patient was discharged to nursing home with nephrostomy catheter and on oral antibiotics (ciprofloxacin). At the 1-month follow-up, the patient was doing well. At this time, there was improvement in the overall condition with down-trending inflammatory markers. A follow-up CT scan was scheduled a month later; however, there was interval worsening of the patient's condition. The patient became drowsy and uncommunicative and the patient's relatives opted for palliative comfort care in an inpatient hospice and no further imaging was performed.
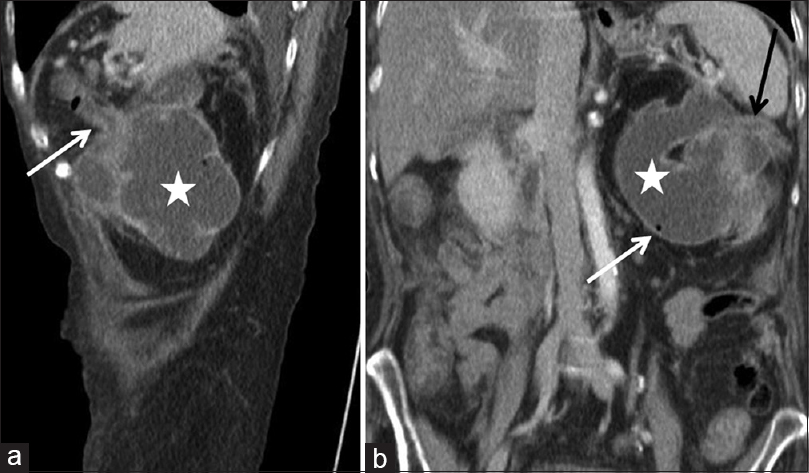
- (a) Oblique sagittal image of computed tomography scan shows dilated left renal pelvis (asterisk) with a reno-colic fistula (white arrow). (b) Coronal computed tomography image shows dilated renal pelvis (asterisk) with an air bubble (white arrow) and reno-colic fistula (black arrow)

- Antegrade pyelography was performed immediately after percutaneous nephrostomy. The injected contrast opacifes the renal pelvis (white arrow) and demonstrates a fistula (arrowhead) with the splenic flexure of the colon (black arrow)
Although first described by Hippocrates, a fistula between renal pelvis and colon is a rare entity. Reno-colic fistula usually results from penetrating trauma and less commonly from diverticular disease, colonic malignancy, or inflammatory bowel disease.[1234] Spontaneous fistula secondary to xanthogranulomatous pyelonephritis, pyonephrosis, and tuberculosis has been described in literature.[567] Our patient was presumed to have a PUJ obstruction and probably developed the fistula from chronic inflammation with superimposed infection, as a diagnosis of exclusion. This is a rather uncommon cause for reno-colic fistula. CT scan shows air in the urinary system in the cases of urinary fistula that can be mistaken for emphysematous infection. Injection of contrast via a nephrostomy catheter is the standard preoperative method to diagnosis reno-colic fistula. This case highlights the utility of multiplanar reconstruction capabilities of modern day CT scanners that can help in diagnosing the reno-colic fistula noninvasively.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Reno-colic arterial fistula due to penetrating abdominal trauma. ANZ J Surg. 2011;81:400.
- [Google Scholar]
- Nephrocolic fistula complicating percutaneous nephrostolithotomy. J Urol. 1988;140:1007-8.
- [Google Scholar]
- An unusual case of pyelonephritis: Nephrocolic fistula owing to a ruptured colonic diverticulum. J Urol. 1974;111:724-6.
- [Google Scholar]
- An unusual case of nephrobronchial and nephrocolonic fistula complicating xanthogranulomatous pyelonephritis. Urology. 1997;50:443.
- [Google Scholar]
- Spontaneous renocolic fistula secondary to calculous pyonephrosis. Urology. 1988;31:147-50.
- [Google Scholar]
- Tubercular renocolic fistula: An unusual presentation. Clin J Gastroenterol. 2012;5:347-50.
- [Google Scholar]




