

Translate this page into:
Acyclovir-induced thrombotic microangiopathy
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Acyclovir is a commonly used antiviral drug. Acute kidney injury (AKI) due to intratubular crystal precipitation and interstitial nephritis is well known. Here we present a case of acyclovir induced AKI in a 61 year old male with herpes zoster, which presented like thrombotic microangiopathy with acute interstitial nephritis. This is the first case report on acyclovir causing thrombotic microaniopathy with partial improvement in renal function after plasmapharesis.
Keywords
Acute kidney injury
acyclovir
thrombotic microangiopathy

Introduction
Acyclovir-induced acute kidney injury (AKI) is a well-documented entity, which is caused due to intratubular crystal precipitation. Selby et al.[1] first reported impaired renal function after treatment with acyclovir in two patients. Numerous case reports and animal studies have described the mechanism of acyclovir nephrotoxicity since the drug was introduced in the 1970s. We present one such case of acyclovir-induced AKI due to thrombotic microangiopathy (TMA) with acute interstitial nephritis. The basis for a diagnosis of acyclovir-induced AKI is supported by clinical features and time course of acyclovir administration.
Case Report
A 61-year-old man came with complaints of painful, unilateral vesicular eruption of 1-week duration in T2 dermatomal distribution due to varicella-zoster virus infection. He received intravenous acyclovir 10 mg/kg 8 hourly for 3 days with a cumulative dose of 4.5 g. Prior to acyclovir administration, his complete blood picture (CBP), hepatic, and renal parameters are normal. After 3 days of administration of acyclovir, he developed anuria, progressive shortness of breath, and peripheral edema. Acyclovir-induced renal dysfunction was contemplated. On investigating, his CBP showed anemia (hemoglobin 8.5 g/dl), thrombocytopenia (platelet count 80,000 cells/mm3), and 5% schistocytes in peripheral smear. Urinalysis showed microscopic hematuria with a mild proteinuria (0.8 g/day) and no evidence of crystals. Renal function test revealed serum creatinine of 6.6 mg/dl with normal electrolyte levels. Lactate dehydrogenase was elevated (840 IU/L) with decreased haptoglobin levels. His liver function tests were normal, and Coomb's test was negative. Autoimmune workup including serum rheumatoid arthritis factor, antinuclear antibody, dsDNA, and antineutrophil cytoplasmic antibodies did not yield positive results. Serum complement levels were normal. HIV, hepatitis A virus, and hepatitis B virus infections were ruled out. ADAMTS13 levels were not studied. Renal biopsy revealed global glomerular capillary thrombosis [Figure 1a–c] with acute interstitial nephritis [Figure 1e and f]. Small arterioles had arteriolar thickening associated with fibrinoid necrosis [Figure 1d] and luminal thrombosis. These features are pathognomonic of arterial TMA. After seven sessions of hemodialysis and three sessions of plasmapheresis, serum creatinine is stable at 4.0 mg/dl with urine output of 1 L/day.
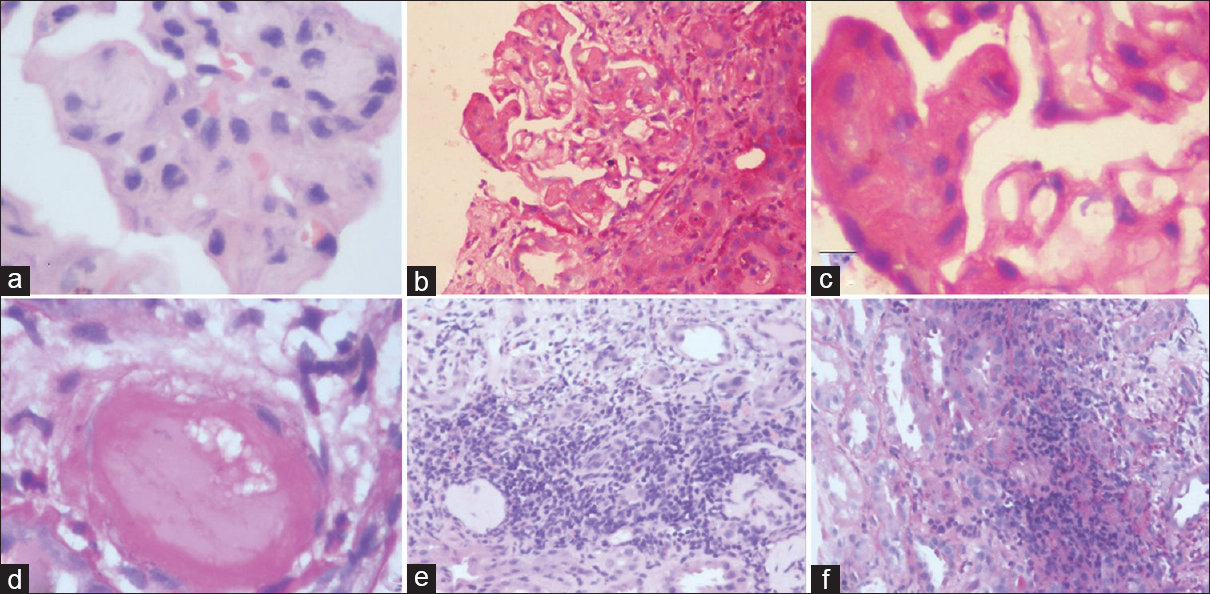
- (a-c) Glomeruli showing intracapillary thrombi. (d) Arteriole showing fibrinoid necrosis of the wall and luminal occlusion by thrombus. (e and f) Interstitum showing dense infiltrate of lymphocytes and neutrophils
Discussion
The main mechanisms of drug-induced nephrotoxicity are vasoconstriction, altered intraglomerular hemodynamics, tubular cell toxicity, interstitial nephritis, crystal deposition, TMA, and osmotic nephrosis. Nephrotoxicity is a well-known side effect of acyclovir, which can occur in 12–48% of patients.[2] Renal failure is typically seen 24–48 h following administration of acyclovir and may be severe.[3] Acyclovir therapy leads to deposition of acyclovir crystals in tubules resulting in tubular obstruction and interstitial inflammation.[4] Birefringent needle-shaped acyclovir crystals can be seen in urine under polarized light. This nephrotoxicity is reversible with early diagnosis and discontinuation of the drug in most of the cases. TMA following administration of mitomycin C and other chemotherapeutic agents like cyclophosphamide appear to be a direct toxicity related to the cumulative dose of the drug. TMA due to acyclovir can be explained by direct drug-induced endothelial damage with concomitant activation of the clotting cascade as the inciting factor[5] or acyclovir-induced antibody formation against the ADAMTS13 enzyme. Fleischer and Johnson suggested that AKI can occur after acyclovir treatment without crystal obstruction from effects on renal microcirculation.[3] There have been suggestions about the possibility of genetic predisposition to the development of nephrotoxicity. Acyclovir has been shown to be a substrate of human organic anion transporter-1 (OAT1) which is present on either side of the renal proximal tubular epithelium. OAT-mediated transport can contribute to two types of renal injury: (i) crystal nephropathy by mediating transepithelial secretion of compounds with low solubility in urine that tend to precipitate upon urinary concentration, such as acyclovir. (ii) Mutations in OAT1 can lead to cytosolic accumulation of acyclovir in renal tissue. Management is largely supportive with adequate hydration and diuretics. Hemodialysis may be required in patients with severe renal failure as in this case. Although there are no reports in the literature to confirm that plasmapheresis is useful in renal recovery, this treatment was utilized in the hope of recovery of renal function.
Conclusion
AKI in patients treated with acyclovir can also be caused due to TMA apart from crystal-induced nephropathy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Parenteral acyclovir therapy for herpesvirus infections in man. Lancet. 1979;2:1267-70.
- [Google Scholar]
- Acyclovir nephrotoxicity: A case report highlighting the importance of prevention, detection, and treatment of acyclovir-induced nephropathy. Case Rep Med. 2010;2010:602783.
- [Google Scholar]
- Acyclovir-induced renal failure. Clinical course and histology. Am J Med. 1988;84:1067-71.
- [Google Scholar]




