

Translate this page into:
Postrenal Transplant Metastatic Colonic Neoplasm: Posttransplant Lymphoproliferative Disorder or Adenocarcinoma?
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Transplant recipients are vulnerable to a horde of infections and neoplastic conditions due to immunosuppression. Posttransplant lymphoproliferative disorder (PTLD) is a condition unique to the transplant recipient occurring due to monoclonal lymphocytic proliferation. It may affect any organ system with reportedly highest incidence in the gastrointestinal tract. The incidence of adenocarcinoma of the colon, however, has not been shown to be uniformly higher in transplant recipients. We report here an unusual case of adenocarcinoma of the ascending colon presenting with liver, lymph node and skin metastasis in a transplant recipient, which simulated PTLD both clinically and radiologically. For any gastrointestinal lesion in transplant recipient, the possibility of carcinoma must be considered. However, a high index of suspicion for PTLD facilitates early diagnosis since the treatment of the two conditions is starkly different.
Keywords
18-fluorodeoxyglucose positron emission tomography-computed tomography
adenocarcinoma colon
posttransplant lymphoproliferative disorder

Introduction
Transplant recipients are susceptible to a variety of neoplasms due to suppression of humoral and cell-mediated immunity. Lymphoproliferative disorders are among the most common posttransplant malignancies. One of the rarest tumors in such patients is colorectal cancer. Posttransplant lymphoproliferative disorder (PTLD) occurring in the colon is difficult to differentiate from adenocarcinoma. Nevertheless, precisely diagnosing PTLD is prudent as it usually responds to reduction of dosage of immunosuppressants and other therapies. We report an unusual case of colonic mass with additional lesions in liver, lymph nodes, and skin in a renal transplant recipient, which initially appeared as PTLD on clinical and radiological evaluation but was subsequently proven to be adenocarcinoma on colonoscopic biopsy.
Case Report
A 60-year-old gentleman underwent live related renal transplantation with the wife as donor in January 2010 for end-stage renal disease secondary to diabetes mellitus and hypertension. His family history was not significant. He was on triple immunosuppression (tacrolimus, prednisolone, and mycophenolate mofetil) and had a nadir creatinine of 1.1 mg/dl. In May 2010, he developed T cell-mediated rejection which was managed with anti-thymocyte globulin and subsequently the patient reached a baseline creatinine of 2.2 mg/dl. He was on regular outpatient follow-up afterwards. In September 2015, he presented with generalized weakness, fatigue, and weight loss for 6 months. There was no history of a decrease in urine output, abdominal pain, or pedal edema. He did not have a history of malena/hematochezia or a history of constipation or loose stools. On examination, blood pressure was 130/88 mmHg, and the patient had severe pallor and mild hepatomegaly. There was no graft tenderness. Hemoglobin was 5.6 g/dl, total leukocyte count (TLC) was 3.5 × 103/μL (normal range: 4–10 × 103/μL), and platelet count was 122 × 103/μL (normal range: 150–400 × 103/μL). Hematological evaluation revealed microcytic hypochromic anemia. Serum albumin was 3.1 g/L. The patient received blood transfusion and erythropoietin for the same after which hemoglobin reached 8.8 g/dl. Ultrasound of the abdomen revealed thickening in the region of the ascending colon along with multiple hypoechoic lesions in both lobes of the liver. 18-fluorodeoxyglucose positron emission tomography-computed tomography (18FDG PET-CT) whole body imaging revealed hypermetabolic lesion in the ascending colon (maximum standardized uptake value [SUVmax] 24.06) along with pericecal and paracolic lymph nodal involvement (SUVmax 7.08), liver involvement (SUVmax 9.29), and subcutaneous deposits in anterior abdominal wall (SUVmax 5.90) suggestive of an extensive disease with multiorgan involvement [Figure 1]. In view of generalized posttransplant disease, a differential diagnosis of posttransplant lymphoproliferative disease and metastatic adenocarcinoma of ascending colon was suggested. Epstein–Barr virus assay was negative. The patient underwent colonoscopy which revealed a circumferential thickening of the ascending colon with 5 cm × 5 cm exophytic growth proximal to the hepatic flexure of colon beyond which the colonoscope was not negotiable [Figure 2a and b]. Biopsy from the growth was suggestive of well-differentiated adenocarcinoma of the colon [Figure 2c and d]. The patient was planned for 5-fluorouracil-based chemotherapy. One week later, he presented with high-grade fever with chills in the absence of other complaints. He was started on broad spectrum antibiotics. On examination, blood pressure was 98/72 mmHg. Hemoglobin was 7.1 g/dl, and serum creatinine was 2.3 mg/dl. TLC was 9.5 × 103/μL. Blood culture and urine culture were sterile. Chest X-ray was suggestive of patches of consolidation in bilateral lower zones. The patient developed Type II respiratory failure for which mechanical ventilation was done. Repeat hematological evaluation was suggestive of persistent pancytopenia likely secondary to pulmonary sepsis. He was started on vasopressor support for hypotension but could not be revived and succumbed to the metastatic disease and sepsis.
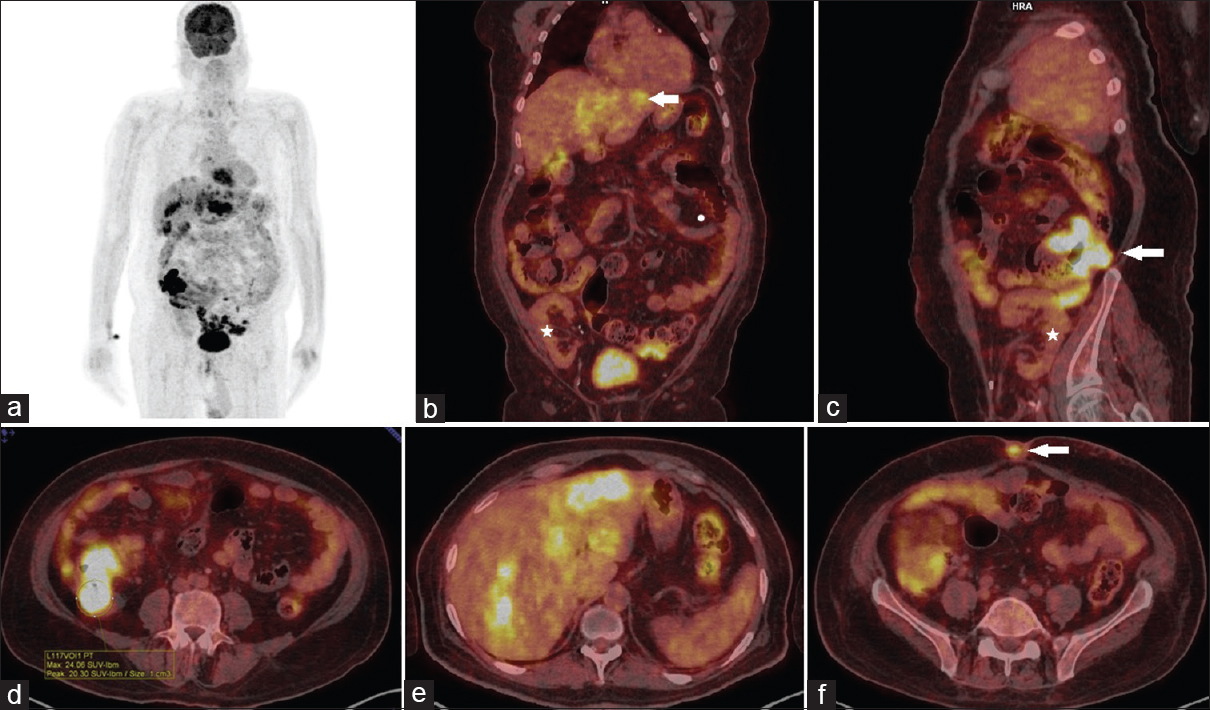
- (a) Coronal positron emission tomography image showing abnormally increased fluorodeoxyglucose uptake in ascending colon and liver, (b) coronal hybrid fluorodeoxyglucose positron emission tomography-computed tomography images reveals transplant kidney (*) with highly active liver metastasis (arrow), (c) sagittal hybrid positron emission tomography-computed tomography images showing graft kidney (*) with fluorodeoxyglucose uptake noted at mass in the caecum and ascending colon (arrow), (d) axial fluorodeoxyglucose hybrid positron emission tomography-computed tomography images show metabolically active mass in the ascending colon (with maximum standardized uptake value 24), (e) axial hybrid fluorodeoxyglucose positron emission tomography-computed tomography images showing highly metabolic multiple liver metastasis, and (f) axial hybrid fluorodeoxyglucose positron emission tomography-computed tomography showing viable soft tissue deposit in the umbilicus (arrow)
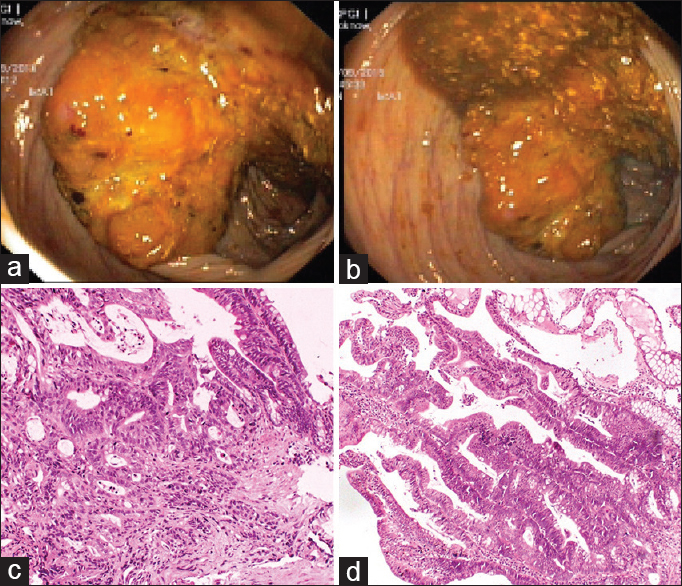
- (a and b) Colonoscopic pictures showing the growth in ascending colon. (c and d) Sections from colonic lesion showing infiltrating tumor disposed in closely packed glandular pattern and lined by tall columnar cells, displaying nuclear stratification and crowding with large vesicular nuclei, prominent nucleoli, and moderate amount of eosinophilic cytoplasm
Discussion
Posttransplant malignancy develops in 20% of patients after 10 years of solid organ transplantation.[1] The most common is skin cancer followed by lymphoproliferative disorders. As kidney is the most common organ to be transplanted, a large number of these cancers occur after renal transplantation.
Most studies conclude that transplant recipients are associated with more aggressive course of colonic adenocarcinoma and may present with widespread metastasis at an early stage.[2345] The symptoms are similar to those seen in nontransplant recipients such as hematochezia, anemia, or symptoms of large bowel obstruction. There is an increased incidence of proximal lesions [6] and right colonic lesions.[7] The aggressive nature of such tumors has been linked to various oncogenic pathways, most importantly the angiogenic and proliferation pathways. KRAS mutations have been proposed as a prognostic marker for colorectal cancer in renal transplant recipients.[8] They have been shown to have predictive role in the targeted therapies such as bevacizumab but their role in the management of such patients is not well defined at present.[9]
The current colorectal cancer screening protocol as well as management is the same as that for the general population.[10] In India, however, routine screening for colorectal cancer is still not performed.[11] Recently, there has been a renewed interest in the screening of colorectal cancer in renal transplant recipients.[3] It has been suggested that patients needing renal transplantation who are 50 years or older must be screened for colorectal cancer [12] and that screening must be done using colonoscopy rather than fecal hemoglobin in such patients.[3]
Surgical resection alone is the standard treatment for localized colonic adenocarcinoma while adjuvant chemotherapy is given for loco-regional disease with lymph node involvement. For a disease with widespread metastasis, aggressive chemotherapy is given to patients with good performance status while a limited therapy and supportive care is preferred for patients with a poor performance status. Surgery in such patients is done only for palliation of symptoms such as obstruction and bleeding.[13]
PTLD usually occur early after transplantation and are related to the degree of immunosuppression and EBV infection. The incidence of PTLD after renal transplantation varies from 1% to 1.5%.[2] The involvement of gastrointestinal tract is seen in one-fifth of the cases and it is the most common extranodal site.[14] Adenocarcinoma of the colon, on the other hand, may not have a higher incidence in transplant recipients compared to the general population, although the disease can be more aggressive.[15]
Clinically, PTLD is suggested by the presence of nonspecific complaints along with hypoalbuminemia, gastrointestinal bleeding, and weight loss. Panendoscopy has been suggested as a useful diagnostic tool for diagnosis of PTLD if there are nonspecific complaints in the absence of definitive gastrointestinal symptoms.[16] The typical colonoscopic appearance of the PTLD lesions is raised rubbery nodular lesions with or without central ulceration. In the present case, the patient had an exophytic growth without raised margins, which is usually a feature of epithelial malignancies, typically adenocarcinoma.
18FDG PET-CT is being increasingly done for aggressive malignancies to assess the extent of the disease before definitive management. Its role in the management of Hodgkin's and non-Hodgkin's lymphoma is well established, and its use in the pretreatment evaluation of PTLD is a natural extension, especially given the frequent extranodal involvement for which CT alone has poor sensitivity.[17] The sensitivity and specificity of 18FDG PET-CT are 89% each, and the SUVmax can be up to 26.4 (median 17.6) for PTLD.[18] For adenocarcinoma of the colon, the median SUVmax is similar, around 16.6.[19] The CT findings of bowel thickening, nodularity and dilatation may be seen in PTLD as well as adenocarcinoma. Hence, for a colonic mass with widespread metastasis such as liver, lymph nodes and skin, PET-CT may not differentiate PTLD from adenocarcinoma, necessitating a colonoscopy for diagnosis.
Conclusion
For renal transplant recipients presenting with nonspecific constitutional symptoms or those with features of gastrointestinal bleeding (overt or covert), there is a high possibility of carcinoma of the colon. Radiological and nuclear imaging does not confirm the diagnosis but can help in assessing the extent of involvement. Early endoscopy and biopsy must be strongly considered to establish the diagnosis as the treatment of other conditions with a similar presentation such as PTLD differs significantly.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The clinicopathologic spectrum of posttransplantation lymphoproliferative disorders. Arch Pathol Lab Med. 2007;131:1209-18.
- [Google Scholar]
- Screening for colorectal cancer and advanced colorectal neoplasia in kidney transplant recipients: Cross sectional prevalence and diagnostic accuracy study of faecal immunochemical testing for haemoglobin and colonoscopy. BMJ. 2012;345:e4657.
- [Google Scholar]
- De novo cancers arising in organ transplant recipients are associated with adverse outcomes compared with the general population. Transplantation. 2009;87:1347-59.
- [Google Scholar]
- A 30-year analysis of colorectal adenocarcinoma in transplant recipients and proposal for altered screening. J Gastrointest Surg. 2007;11:272-9.
- [Google Scholar]
- Importance of pre-transplant colonoscopy in renal transplant recipients. J Clin Med Res. 2014;6:414-21.
- [Google Scholar]
- Cancer risk following organ transplantation: A nationwide cohort study in Sweden. Br J Cancer. 2003;89:1221-7.
- [Google Scholar]
- Role of oncogenic pathways and KRAS/BRAF mutations in the behavior of colon adenocarcinoma in renal transplant patients. Transplantation. 2012;93:509-17.
- [Google Scholar]
- New strategies for treatment of KRAS mutant metastatic colorectal cancer. Clin Cancer Res. 2010;16:2921-6.
- [Google Scholar]
- Canadian Society of Transplantation: Consensus guidelines on eligibility for kidney transplantation. CMAJ. 2005;173:S1-25.
- [Google Scholar]
- Yield of screening colonoscopy in renal transplant candidates. Can J Gastroenterol Hepatol. 2015;29:423-6.
- [Google Scholar]
- Cancer of the colon. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. DeVita, Hellman, and Rosenberg's Cancer: Principles & Practice of Oncology. Philadelphia, United States: Wolters Kluwer; 2015. p. :783-95.
- [Google Scholar]
- Abdominal-pelvic lymphoproliferative disease after lung transplantation: Presentation and outcome. Transplantation. 2004;77:431-7.
- [Google Scholar]
- The involvement of the gastrointestinal tract in posttransplant lymphoproliferative disease in pediatric liver transplantation. J Pediatr Gastroenterol Nutr. 1999;28:380-5.
- [Google Scholar]
- Positron emission tomography scanning in the setting of post-transplant lymphoproliferative disorders. Clin Transplant. 2009;23:794-9.
- [Google Scholar]
- The accuracy of positron emission tomography in the detection of posttransplant lymphoproliferative disorder. Haematologica. 2013;98:771-5.
- [Google Scholar]
- Incidental colonic focal FDG uptake on PET/CT: Can the maximum standardized uptake value (SUVmax) guide us in the timing of colonoscopy? Eur J Nucl Med Mol Imaging. 2015;42:66-71.
- [Google Scholar]




