

Translate this page into:
Role of Preoperative Duplex Ultrasonography to Predict Functional Maturation of Wrist Radiocephalic Arteriovenous Fistula: A Study on Indian Population
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Radiocephalic arteriovenous fistula (RCAVF) is the first choice for native arteriovenous fistula (AVF). Preoperative vessel assessment with ultrasonography (USG) has been reported to enhance the outcome of native AVF, but data regarding its predictive value for functional maturation of RCAVF are scanty. We aimed to determine the role of preoperative duplex USG (DUS) for prediction of functional maturity of radiocephalic fistula in the wrist. The data from 173 patients were analyzed prospectively. The estimated duplex variable included size, patency, and continuity of cephalic vein and size, peak systolic velocity, and wall calcifications in radial artery at the wrist. The subjects underwent RCAVF creation and were reviewed 6–8 weeks post procedure for adequacy of maturation. Doppler variables between successful and failed maturation groups were compared. Successful functional fistula maturation was noted in 138 (80.9%) patients. Values of radial artery diameter, cephalic vein diameter, and peak systolic velocity were >2 mm, 2.2 mm, and 32.8 cm/s, respectively, for successful maturation of RCAVF in more than 90% of cases. Vascular calcifications were detected preoperatively in 15 diabetic patients and 9 (60%) of them had fistula failure. Preoperative DUS can provide a good prediction on functional maturation of RCAVF. Vascular calcifications were associated with high risk of maturation failure in diabetics.
Keywords
Arteriovenous fistula
duplex ultrasonography
hemodialysis access
maturation of arteriovenous fistula

Introduction
The native arteriovenous fistula (AVF) is the preferred modality for hemodialysis access due to a lower rate of thrombosis, infection, need for secondary interventions compared to grafts, as well as longer survival and functional patency rates.[1] The National Kidney Foundation-Kidney Disease Outcome Initiative recommends wrist radiocephalic AVF (RCAVF) as the first choice for native AVF.[2] Despite the known higher incidence of failed maturation for radiocephalic fistulas, the ease of placement and the preservation of proximal vessels for future access outweigh such disadvantages.[3] The most important factors for the successful outcome of fistula surgery and adequate fistula flow are adequate arterial volume flow, patency, and adequate distension capacity of the vein. In the early postoperative period, the presence of spiral laminar flow pattern on Doppler in outflow vein has been considered as the most important and earliest factor in predicting the maturation of AVF.[4] Preoperative vessel assessment with ultrasonography (USG) enhances the success of creation and outcome of native AVF.[3] Malovrh has demonstrated a good correlation with arterial and venous diameters with actual measured values.[5] Attempts have been made by various authors, to analyze preoperative duplex variables predicting successful functional maturation of RCAVF, but there is a scarcity of prospective studies in this regard, especially in the Indian scenario. Hence, we have designed this study prospectively to determine the role of preoperative duplex USG (DUS) for prediction of functional maturity of radiocephalic fistula in the wrist in North Indian populations.
Materials and Methods
After obtaining approval from the Institutional Review Board, 186 patients diagnosed with end-stage renal disease and referred for permanent hemodialysis access by nephrologist were prospectively enrolled in the study from October 2011 to June 2015. Informed consent was obtained from all patients before enrolment. Patient enrolment was done after stringently adhering to exclusion criteria. All patients underwent a preoperative physical examination of the vascular system. Arterial assessments included pulse examination, blood pressure measurements in both upper limbs, and the Allen's test for continuity of the palmar arch. Venous assessments included gross evaluation of veins in dependent position with tourniquet enhancement in the upper arm. All patients were subjected to preoperative DUS of arteries and veins of both upper limbs. This noninvasive imaging was done using 5, 6, or 12 MHz scanning probes by an experienced vascular radiologist. Estimated duplex variables included diameter, patency, and continuity of cephalic vein and size, peak systolic velocity, and vessel wall calcification in radial artery at the wrist.
Exclusion criteria
-
The subjects with attenuated and no demonstrable flow in radial arteries
-
The subjects with thrombosed cephalic vein on duplex
-
Those patients with no palpable thrill or murmur postprocedure to remove confounding factor of technical error
-
Patients who underwent preemptive fistula surgery for future dialysis.
A total of 13 patients were excluded from the study after subjecting to surgery. In five patients, the cephalic vein was attenuated deterring an arteriovenous anastomosis. In rest of 8 patients who were excluded, there was no palpable thrill or murmur post procedure. The subjects underwent RCAVF creation at a level just proximal to the wrist. All surgeries were done by an experienced vascular surgeon or a senior registrar under his supervision. Arteriotomies were standardized to 1 cm and venotomy to 1.4 cm (unstretched venous length). All anastomoses were done in an end-to-side manner with running 6’0’ polypropylene. Patients were then seen routinely 7–14 days postoperatively and at 6–8 weeks thereafter to assess for adequate maturation. If fistula appeared matured on physical examination, the first dialysis through fistula was given. During dialysis, maximum flow provided by the fistula was measured. In those patients with inadequate dilatation for a successful puncture, another 2 weeks were given for further dilatation.
Criteria for successful maturation
The criterion for successful maturation of fistula was defined as:
-
Easily obtainable puncture
-
Successful dialysis >4 h through fistula on 3 or more consecutive occasions
-
A fistula, which provides minimum blood flow of 300 ml/min or more for 4 h.
Data collection and statistical analysis
All data were recorded in a performa specifically designed for the study. Demographic data such as age, gender in addition to comorbidities such as diabetes, hypertension, and tobacco use were documented. All duplex parameters described earlier were recorded in the same data sheet. Data analysis was done using SPSS 16 (SPSS Inc., Chicago, IL, USA). Independent t-test was used to compare means of Doppler variables between subjects with successful and failed maturation as well as diabetics and non-diabetics with maturation failure. Chi-square test and Fisher exact test were used to compare outcomes between groups. Discriminate function analysis was done to generate a cutoff value for Doppler variables associated with successful functional maturation. P value of <0.05 was considered significant.
Results
The data of 173 patients (121 males and 52 females) were analyzed. The mean age in this cohort was 43.3 ± 11.5 years (range 16–69 years). Thirty-three patients (19.1%) were diabetic (mean age 45.5 ± 5.5). Prior history of RCAVF failure on opposite hand was present in 8 (4.6%) patients.
On duplex scan, mean radial artery and cephalic vein diameter (CVD) were 2.27 ± 0.66 mm (range 1.4–3 mm) and 2.24 ± 0.33 mm (range 1.6–3.7 mm), respectively. Mean peak systolic velocity (PSV) in radial artery was 54.76 ± 17.6 cm/s (range 15.7–92.5 cm/s).
Successful functional fistula maturation was noted in 138 (80.9%) patients. Among 35 patients with maturation failure, 22 patients did not have any evidence of flow through the fistula whereas rest had a flow rate inadequate to support dialysis.
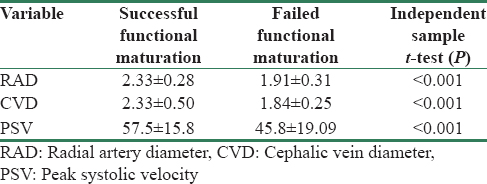
The means of radial artery diameter (RAD), CVD, and PSV with successful and failed functional maturation groups were compared. On independent sample t-test, the means of the above-mentioned three variables were significantly different between the two groups [Table 1].
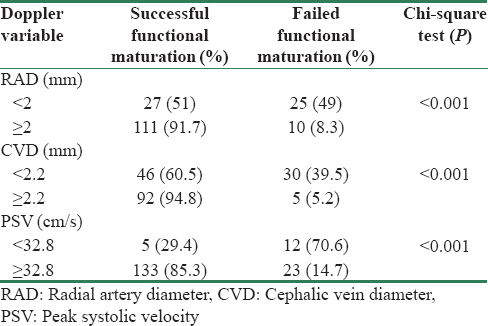
On discriminate function analysis, the cutoff values associated with successful functional maturation were 2 mm, 2.2 mm, and 32.8 cm/s for RAD, CVD, and PSV, respectively. The subjects were stratified based on cutoff value with respect to each variable and compared using Chi-square test. The functional maturation was significantly different between groups above and below cutoff values with respect to each Doppler variable [Table 2].
Vascular calcification was detected preoperatively in 17 patients and was positively correlated with intraoperative finding. The majority of them (15 patients) were diabetics. Of these, 9 (52.3%) had fistula failure and all were diabetics. On Chi-square test for independence, calcification as a variable was associated to be having high chance of failure for functional maturation with P - 0.001 which was statistically significant.
Among 33 patients with diabetes, 17 (51.5%) had fistula failure. On comparison with non-diabetic patients, risk of maturation failure was statistically significant (P < 0.00). Duplex parameters were compared between diabetic and non-diabetic categories with fistula maturation failure [Table 2]. On applying independent t-test, mean CVD and mean PSV were not significantly different between two categories. The difference between mean RAD was statistically significant between two groups (P - 0.03) [Table 3]. Arterial calcifications in diabetic patients were associated with decreased rate of functional maturation of AVF. Of 17 diabetics with fistula maturation failure, 9 (52.9%) had presence of arterial calcification on preoperative duplex. On applying Fisher's exact test between non-diabetic and diabetic categories with fistula maturation failure for the presence of calcification, P value shown was < 0.001 which is highly significant.

On subgroup analysis, 103 (85.1%) males had successful outcome out of 121 patients while procedure was successful in 35 (67.3%) of 52 female patients. Both these groups were compared, and this difference was statistically significant (Chi-square value 0.007). The history of prior fistula failure was not associated with any significant difference in future fistula maturation.
Discussion
The native AVFs are associated with superior overall patency, lower revision rate, and cost savings, compared with prosthetic arteriovenous grafts.[6] A visual inspection and physical examination of the upper extremity alone may be inadequate to assess the quality of arterial inflow and continuity of venous outflow.[789] The role of Doppler to define the presence of spiral laminar flow pattern in outflow vein following creation of fistula has been established as the earliest postoperative parameter in predicting maturation as reported by Srivastava et al.[4] Similarly, Doppler USG has a role to play in preoperative vessel assessment to predict the success of creation and the outcome of native AVF.[3] Mihmanli et al., in a randomized trial, have reported 25% primary AVF failure rate when preoperative assessment depended on physical examination alone, compared with 6% when USG was used.[8] Patients with a RAD of 2 mm and a CVD of 2.5 mm received RCAVF.[9] This prospective study was conducted to analyze how Doppler variables predict functional maturation of RCAVF.
In the present group, 138 (80.8%) patients had successful functional fistula maturation by 6–8 weeks post-procedure. Lauvao et al., in their series, have reported a 66% functional maturation in RCAVF.[7] Mihmanli et al. have reported a success rate of 75% in their series of 52 patients[8]. The early failure rate described for wrist RCAVFs varies from 5% to 30%.[1011] The functional maturation observed in this cohort is well comparable to the above-said reports.
In the present study, Doppler parameters significantly differed between patients with successful or failed functional maturational outcome. Mean RAD noted in our patients with successful outcome versus maturation failure was 2.33 ± 0.28 and 1.91 ± 0.31 mm, respectively. This difference was also statistically significant when means were compared using independent t-test (P < 0.00). On discriminant function analysis, value for RAD associated with successful maturation in >90% was 2 mm. An earlier study by Lemson et al. has reported that successful RCAVFs had a preoperatively measured RAD of 2.7 versus 1.9 mm in failed RCAVFs.[11] This decreased trend in functional maturation of RCAVFs with decreased radial artery size has been reported by several authors.[3] Wong et al. had observed early failure in RCAVFs created in patients with a RAD of <1.6 mm.[12] Malovrh discriminated between RCAVFs created with radial arteries, with a diameter >1.5 mm versus <1.5 mm.[5] Immediate patency rate in the >1.5 mm group was 92% versus 45% in the <1.5 mm group, while the patency rates after 12 weeks were 83% versus 36%, respectively. The RAD for successful maturation was relatively higher in our study may be because of the fact that we have considered maturation in terms of successful hemodialysis as an end-point rather than patency rate or early failure rate. More so, discriminant function analysis of this study was done keeping the success rate of >90% which was higher than other contemporary study.
The predictive value of the radial artery PSV calculated from preoperative ultrasonographic parameters is uncertain.[1213] In our cohort, radial artery mean PSV noted in successfully matured and failed groups was 57.5 ± 15.8 and 45.8 ± 19.0 cm/s, respectively, and this difference was also statistically significant (P < 0.001). The cutoff value revealed by discriminant analysis was 32.8 cm/s.
Lauvao et al. have reported vein size as the major predictive factor in fistula functional maturation in RCAVF as well as BCAVF.[7] Vein diameters of <1.6 mm have been associated with AVF failure,[12] while good patency rates were obtained in patients with RCAVFs where the diameter of the cephalic vein at the wrist was >2–2.6 mm.[14] In the present group of patients, mean cephalic vein size noted was significantly different between functionally matured and failed fistula (2.33 ± 0.50 vs. 1.84 ± 0.25). This difference of means was also statistically significant (P < 0.001). The CVD cutoff estimated using discriminant analysis, associated with successful functional maturation of >90% in our series, was 2.2 mm.
The presence of diabetes and concomitant arteriosclerosis may have an additional negative impact on the chance of successful access creation.[15] Diabetes mellitus and arteriosclerosis are now the most important causes for dialysis treatment.[3] These patients usually have poor, thickened, and calcified arteries with proximal and/or distal vessel obstruction.[16171819] Multiple authors have reported poor results with native fistulae in diabetics.[1718] In our study group, 33 patients had diabetes and 17 (51.5%) had fistula failure, and this result was statistically highly significant (Chi-square test, P < 0.001). Konner et al. have reported the incidence of primary RCAVF rates of 23% in diabetics versus 62% in non-diabetics.[19] Multiple authors have reported disappointing results with wrist fistulae and achieved better results with proximal fistulae in diabetic patients.[20] In this study, the diabetic population was 19% which appears to be low, this may be because of the fact that many diabetic patients were not enrolled in view of attenuated and no demonstrable flow in radial arteries and considered for proximal fistula.
The differences in duplex variables were compared between diabetics to non-diabetic patients [Table 2]. Radial artery diameter showed a significant difference between diabetics with failed maturation and non-diabetics with failed maturation (independent t-test, P - 0.03). Other variables such as CVD and PSV were not significantly different between two groups. The incidence of arterial calcification was higher in diabetic group (52.9%). Of 17 diabetics with fistula maturation failure, 9 patients had presence of arterial calcification. On applying Fisher's exact test between non-diabetic and diabetic categories with fistula maturation failure for presence of calcification, P value shown was < 0.001, which is highly significant. Multiple authors have reported a high incidence of radial artery calcifications in diabetic patients.[2122] Allon et al. have advocated in their study to avoid arteries with calcified arterial wall as it is associated with low maturation of fistula.[23] One reason cited for this phenomenon is an inadequate vasodilatory response in arteries with calcified and sclerosed media. Konner has reported a proximal approach more successful in this subset of patients.[24]
Even though this study was designed prospectively, certain limitations need to be highlighted. Confounding factors such as duration of CKD, duration of hypertension, smoking status had not been taken into consideration, which might have some impact on the outcome of AVF.
Conclusion
The preoperative DUS can provide a reasonable prediction of functional maturation of RCAVF. The present study proposes a RAD, CVD, and radial artery PSV of 2 mm, 2.2 mm, and 32.8 cm/s, respectively, for a high rate of successful functional maturation of RCAVFs. Vascular calcifications were associated with high risk of maturation failure in diabetics. Proximal fistulas should be considered in diabetic patients with inadequate arterial diameter and calcifications.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: Hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis. 2006;48(Suppl 1):S1-322.
- [Google Scholar]
- Spiral laminar flow, the earliest predictor for maturation of arteriovenous fistula for hemodialysis access. Indian J Urol. 2015;31:240-4.
- [Google Scholar]
- Non-invasive evaluation of vessels by duplex sonography prior to construction of arteriovenous fistulas for haemodialysis. Nephrol Dial Transplant. 1998;13:125-9.
- [Google Scholar]
- Cost analysis of ongoing care of patients with end-stage renal disease: The impact of dialysis modality and dialysis access. Am J Kidney Dis. 2002;40:611-22.
- [Google Scholar]
- Vein diameter is the major predictor of fistula maturation. J Vasc Surg. 2009;49:1499-504.
- [Google Scholar]
- Cephalic vein and hemodialysis fistula: Surgeon's observation versus color Doppler ultrasonographic findings. J Ultrasound Med. 2001;20:217-22.
- [Google Scholar]
- A strategy for increasing use of autogenous hemodialysis access procedures: Impact of preoperative noninvasive evaluation. J Vasc Surg. 1998;27:302-7.
- [Google Scholar]
- Comparison of autogenous fistula versus expanded polytetrafluoroethylene graft fistula for angioaccess in hemodialysis. Am J Surg. 1986;152:238-43.
- [Google Scholar]
- Does pre-operative duplex examination improve patency rates of Brescia-Cimino fistulas? Nephrol Dial Transplant. 1998;13:1360-1.
- [Google Scholar]
- Factors associated with early failure of arterio-venous fistulae for haemodialysis access. Eur J Vasc Endovasc Surg. 1996;12:207-13.
- [Google Scholar]
- Preoperative sonographic radial artery evaluation and correlation with subsequent radiocephalic fistula outcome. J Ultrasound Med. 2004;23:161-8.
- [Google Scholar]
- Utility of ultrasonographic venous assessment prior to forearm arteriovenous fistula creation. Clin Nephrol. 2002;58:122-7.
- [Google Scholar]
- Predictors of type of vascular access in hemodialysis patients. JAMA. 1996;276:1303-8.
- [Google Scholar]
- Preexisting intimal hyperplasia of radial artery is associated with early failure of radiocephalic arteriovenous fistula in hemodialysis patients. Am J Kidney Dis. 2003;41:422-8.
- [Google Scholar]
- Prosthetic fistula survival and complications in hemodialysis patients: Effects of diabetes and age. Am J Kidney Dis. 1992;19:448-52.
- [Google Scholar]
- The arteriovenous fistula for hemodialysis access: Gold standard or archaic relic? Am Surg. 1996;62:652-6.
- [Google Scholar]
- Tailoring the initial vascular access for dialysis patients. Kidney Int. 2002;62:329-38.
- [Google Scholar]
- Increased incidence of radial artery calcification in patients with diabetes mellitus. J Surg Res. 2002;102:1-5.
- [Google Scholar]
- Hemodialysis access placement with preoperative noninvasive vascular mapping: Comparison between patients with and without diabetes. Am J Kidney Dis. 2001;38:560-4.
- [Google Scholar]
- Factors associated with prevalence of arterio-venous fistulae in haemodialysis patients in the HEMO study. Kidney Int. 2000;58:2178-85.
- [Google Scholar]
- Primary vascular access in diabetic patients: An audit. Nephrol Dial Transplant. 2000;15:1317-25.
- [Google Scholar]




