

Translate this page into:
Perinuclear Antineutrophil Cytoplasmic Antibody Positive Glomerulonephritis in a Case of Limited Cutaneous Scleroderma
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Antineutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis in a patient of scleroderma is very rare. Very few cases have been reported in English literature. We report a case of a 58-year-old male with long-standing limited cutaneous scleroderma (Scl-70 positive) presenting with normotensive scleroderma renal crisis. Perinuclear ANCA with antimyeloperoxidase antibody was found to be strongly positive. Renal biopsy showed pauci immune-necrotizing crescentic glomerulonephritis. We believe that this case report will be helpful in understanding clinical features of normotensive ANCA-associated glomerulonephritis in scleroderma patients.
Keywords
Antineutrophil cytoplasmic antibody
glomerulonephritis
scleroderma

Introduction
Systemic sclerosis (SSc) is a chronic systemic fibrozing disease. The main manifestations are attributed to 3 features - tissue fibrosis, microvascular injury, and autoimmune disorder.[1] Renal involvement in scleroderma occurs mainly in the form of scleroderma renal crisis (SRC), affecting 5%–10% of the patients. Other renal pathologies in scleroderma include scleroderma overlap syndromes with associated features of lupus nephritis, anti-myeloperoxidase (MPO), or anti PR-3 antineutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis or crescentic glomerulonephritis. These alternative pathologies should be suspected in any patient with a differing clinical picture and the patient should be appropriately investigated. In scleroderma, the vascular abnormalities are considered to be noninflammatory. Vasculitis in scleroderma has been reported only rarely.
The clinical significance and prognosis of ANCA-associated vasculitis (AAV) in SSc are not well known. It is also unclear whether vasculitis occurs more frequently in patients with limited versus diffuse cutaneous variants of SSc. The objective is to report a case of scleroderma with perinuclear ANCA (P-ANCA)-associated glomerulonephritis and to compare the clinical characteristics of this patient with other ANCA-associated scleroderma cases.
Case Report
A 58-year-old male diagnosed with limited cutaneous scleroderma for 5 years (ANA positive, anti Scl-70 positive), presented with abnormal renal parameters (raised serum creatinine 2.7 mg/dl, hematoproteinuria) on routine investigations. He had a history of Raynaud's phenomenon for 20 years and digital ulcers for 7 years. He did not have any interstitial lung disease or pulmonary hypertension. On examination, there was depigmentation of the scalp, skin tightening of the face, telangiectasia, pitting scars, and sclerodactyly. His vital parameters were stable on admission with a pulse of 80/min, blood pressure (BP) 120/80 mmHg, and normal oxygen saturation. Urine analysis showed hematoproteinuria (urine protein/creatinine ratio = 0.6, red blood cells = 40–50/high power field) while the serum creatinine was 2.7 mg/dl. His complement levels were normal (C3 = 86.9, C4 = 13.10). ANA profile showed a positive result for Scl-70 with all the other antibodies being negative. P-ANCA was positive and the MPO-ANCA titers were significantly elevated at >200 IU/ml. Light microscopy of the renal biopsy revealed 10 out of 14 glomeruli showing complete and partial cellular/fibrocellular crescents. The underlying glomerular capillary loops were compressed and showed focal areas of fibrinoid necrosis. Interstitium showed mild chronic inflammation and focal areas of fibrosis. Vessels were unremarkable.[Figures 1 and 2]. Immunofluorescence did not reveal any positivity for immune deposits supporting the diagnosis of pauci immune (P-ANCA associated) necrotizing crescentic glomerulonephritis. He was given three doses of pulse methylprednisolone therapy (500 mg each) followed by injection cyclophosphamide 500 mg one dose during the same admission and advised to continue regular follow-up. He received 6 doses of cyclophosphamide followed by maintenance therapy with mycophenolate mofetil 1 g/day and oral prednisolone. His current serum creatinine is 1.34 mg/dl.
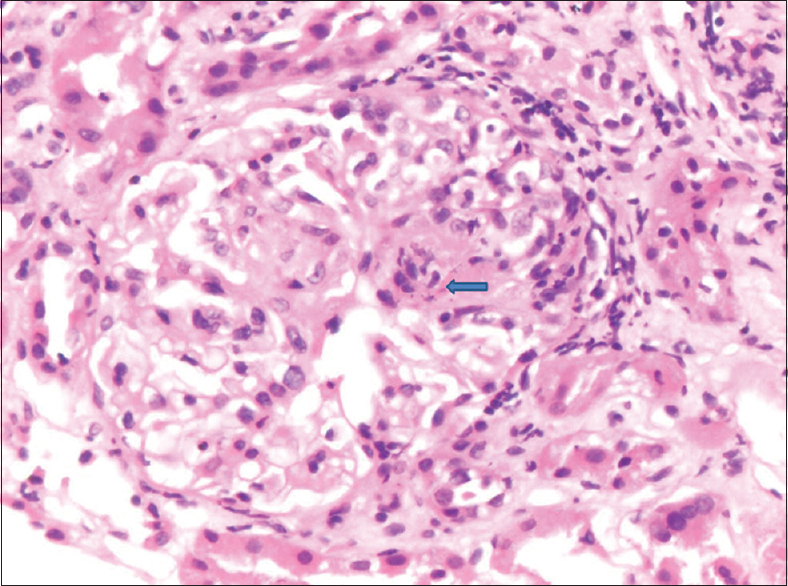
- ×40 glomerulus showing a partial fibrocellular crescent. A segmental area of necrosis is noted (arrow). The underlying glomerulus is compressed. The interstitium shows mild fibrosis and a chronic inflammatory infiltrate

- ×40 glomerulus is almost completely replaced by a fibrocellular crescent showing areas fibrinoid necrosis (arrows). The interstitium shows fibrosis
Discussion
SRC is a well-known complication of scleroderma. It usually occurs early in the course of scleroderma and is characterized by rapidly progressive renal failure, elevated plasma renin activity, and malignant hypertension. It is more common in diffuse cutaneous type of scleroderma.[2] In 1989, Helfrich et al. first reported 131 patients who developed SRC, but 15 of them did not have malignant hypertension.[3] In 1994, Endo et al. first reported renal failure without malignant hypertension in a scleroderma patient who was MPO-ANCA positive.[4] This led to the recognition of normotensive renal failure in scleroderma. It is after 1994 that reports of ANCA-related crescentic glomerulonephritis in scleroderma have been published, possibly due to easy availability of ANCA testing. In Japanese literature, 22 cases of ANCA related or normotensive renal failure with scleroderma have been reported.
Quéméneur et al. have reported the prevalence of vasculitis in SSc patients as <1%.[5] Three other studies have shown prevalence close to their estimation, ranging between 0% and 1.3%. No SRC has been seen in the previously reported cases despite the use of high doses of corticosteroids. This could be related to AAV being more prevalent in patients with limited cutaneous type of SSc. Interestingly, 97% of SSc patients with cooccurrence of AAV were serologically positive for p-ANCA and MPO antibodies. There is only 1 report of a patient with SSc and AAV (c-ANCA) with clinical features of granulomatosis with polyangiitis (nasal inflammation, lung opacity, and crescentic pauci immune glomerulonephritis). Liang and Michet in a recent series of fourteen patients with scleroderma and ANCA vasculitis found majority of patients to have limited scleroderma.[6]
There are clinical and histopathological differences in both types of renal failure. Patients with normotensive renal failure usually do not present with malignant hypertension, fluid overload, or high renin levels.[7] Alveolar hemorrhages are more common in ANCA-related renal failure. In English literature, 58 cases of normotensive SRC have been reported. The characteristics of AAV with scleroderma are described as being most common in the fifth and sixth decade of life (mean age 57) and the male to female ratio as 1:4, similar to the general gender distribution of all SSc patients. The average duration of SSc until the appearance of overt AAV is about 9 years. In the AAV cohort, positive serology for Scl-70 was common (77%), while the frequency of this antibody within SSc in general is usually around 25%. In addition, it was observed that SSc was mainly of the limited cutaneous type.[8] Arad et al. has recently presented a case series of three patients and has supported previous associations of significant pulmonary hemorrhage associated with AAV and scleroderma.[9] Rho et al. suggested that anti-Scl-70 antibodies could play a role in the development of AAV in SSc patients and could be a significant predictor for the development of AAV in SSc patients.[10]
In our case, the patient is a male, without any pulmonary involvement and renal disease was detected 5 years after the diagnosis of scleroderma, which is earlier as compared to most other case reports.
Thus, in our case, some of the characteristics of AAV patients were slightly different.
Conclusion
Our case reinforces the occurrence of AAV in patients with SSc. ANCA testing and kidney biopsy should be performed in patients of SSc with renal involvement, normal BP, and the absence of microangiopathic hemolytic anemia. Prompt recognition of vasculitis could lead to the early introduction of an appropriate immunosuppressive regimen resulting in better renal and global survival.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A case of progressive systemic sclerosis with crescentic glomerulonephritis associated with myeloperoxidase-antineutrophil cytoplasmic antibody (MPO-ANCA) and anti-glomerular basement membrane antibody (anti-GBM Ab) Nihon Jinzo Gakkai Shi. 1995;37:207-11.
- [Google Scholar]
- Hypertension and renal failure (scleroderma renal crisis) in progressive systemic sclerosis. Review of a -year experience with cases. Medicine (Baltimore). 1983;62:335-52.
- [Google Scholar]
- Normotensive renal failure in systemic sclerosis. Arthritis Rheum. 1989;32:1128-34.
- [Google Scholar]
- Antineutrophil cytoplasmic autoantibodies in 6 patients with renal failure and systemic sclerosis. J Rheumatol. 1994;21:864-70.
- [Google Scholar]
- Systemic vasculitis during the course of systemic sclerosis: Report of 12 cases and review of the literature. Medicine (Baltimore). 2013;92:1-9.
- [Google Scholar]
- ANCA associated vasculitis in scleroderma: A case series of fourteen patients. Rheumatol Rep. 2011;3:3-8.
- [Google Scholar]
- Revisiting ANCA-associated vasculitis in systemic sclerosis: Clinical, serological and immunogenetic factors. Rheumatology (Oxford). 2013;52:1824-31.
- [Google Scholar]
- ANCA-related cresentic glomerular nephritis in a patient with scleroderma without marked dermatological changes and malignant hypertension. Intern Med. 2004;43:496-502.
- [Google Scholar]
- Anti-neutrophil antibody associated vasculitis in systemic sclerosis. Semin Arthritis Rheum. 2011;41:223-9.
- [Google Scholar]
- Scleroderma associated with ANCA-associated vasculitis. Rheumatol Int. 2006;26:369-75.
- [Google Scholar]




