

Translate this page into:
Successful Treatment of Renal Infiltration Complicated by Atypical Hemolytic Uremic Syndrome in a Leukemic Child
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Renal infiltration in children with acute leukemia has been reported previously; however, it has rarely been described in association with atypical hemolytic uremic syndrome (aHUS). We present a case of 9-year-old boy who developed life-threatening aHUS in the 1st week of Burkitt leukemia/lymphoma diagnosis with renal infiltration. Complete resolution of aHUS was achieved after therapeutic plasma exchange. This is an uncommon complication of Burkitt leukemia/lymphoma in a pediatric case.
Keywords
Hemolytic uremic syndrome
leukemia
lymphoma

Introduction
Renal infiltration in children with acute leukemia has been reported previously; however, it has rarely been described in association with atypical hemolytic uremic syndrome (aHUS).[12345678] Most reported cases of aHUS have been diagnosed either before the first signs of leukemia or after chemotherapy for leukemia.[2345678] A literature search revealed only one case of simultaneous occurrence of aHUS and acute lymphoblastic leukemia (ALL) till date.[2] We report the first case of the therapeutic plasma exchange (TPE) treatment in a child with precursor type t(8;14)(q24;q32)-positive Burkitt leukemia/lymphoma who had renal infiltration complicated by aHUS.
Case Report
A 9-year-old boy presented with oliguria, hypertension, and periorbital edema. He was diagnosed with precursor type t(8;14)(q24;q32)-positive Burkitt leukemia/lymphoma with central nervous system involvement and tumor lysis syndrome (TLS). A complete blood count showed hemoglobin (Hb) concentration 8.3 g/L and platelet count 43 × 109/L. Biochemical investigations revealed elevated uric acid (9 mg/dl) and lactate dehydrogenase (LDH; 2400 IU/L). The patient's electrolyte imbalance resolved, but his urine output remained inadequate despite effective hydration and hemodialysis for TLS. Radiological imaging and urinalysis suggested renal infiltration secondary to acute leukemia. Macroscopically, the patient's urine resembled lipemic plasma and microscopic examination revealed abundant blast cells. These observations were supported by positron emission tomography (PET) and magnetic resonance imaging (MRI) findings consistent with renal infiltration, including bilateral renal enlargement and pathological increased uptake of 18F-fluoro-2-deoxy-D-glucose [Figure 1a]. Epstein-Barr virus polymerase chain reaction was negative at diagnosis. His urinary findings and immunophenotypic features were previously reported by Kaya et al.[9]

- Initial and posttreatment 18F-fluoro-2-deoxy-D-glucose positron emission tomography images. On the initial positron emission tomography scan (a) diffuse increased 18F-fluoro-2-deoxy-D-glucose uptake was observed in bone marrow, renal parenchyma and the enlarged spleen suggesting diffuse malignant cell infiltration in these organs. The posttreatment positron emission tomography examination (b) showed normal distribution of 18F-fluoro-2-deoxy-D-glucose and complete resolution of previous pathological positron emission tomography findings
While on steroid therapy, the patient's LDH (19,536 IU/L) and creatinine (2.32 mg/dl) levels increased markedly again and his anemia and thrombocytopenia worsened despite transfusion on day 7 [Figure 2a]. At that time, his Hb, platelets and reticulocytes were 4.9 g/dl, 26.8 × 109/l and 6.5%, respectively. His peripheral blood examination consisted with microangiopathic features such schistocytes and helmet cells [Figure 2b]. His coagulation profile was normal and direct Coombs test was negative. Urinalysis showed hematuria and his haptoglobin level was below 10 mg/dl (normal range: 30–200 mg/dl). His ADAMTS-13 activity and stool tests were normal, but his C3 level was 77 mg/dl (79–152 mg/dl). He developed aHUS in the 1st week after diagnosis. Acute renal failure did not respond to 10–15 cc/kg fresh frozen plasma infusion and steroid administration. TPE was administered for 2 consecutive days, after which clinical and laboratory assessments revealed a dramatic response. Induction chemotherapy was continued without any complications, and he was in complete remission on day 33. The patient remained well with no signs of disease recurrence in PET and MRI imaging during 2 months after diagnosis [Figure 1b]. However, on day +70, while still on the second induction phase, he developed very early combined bone marrow and central nervous system relapse. The second complete remission was achieved with ALL-REZ BFM-2002 protocol and rituximab. At the time of writing, allogeneic hematopoietic stem cell transplant was scheduled from full-matched sibling donor.
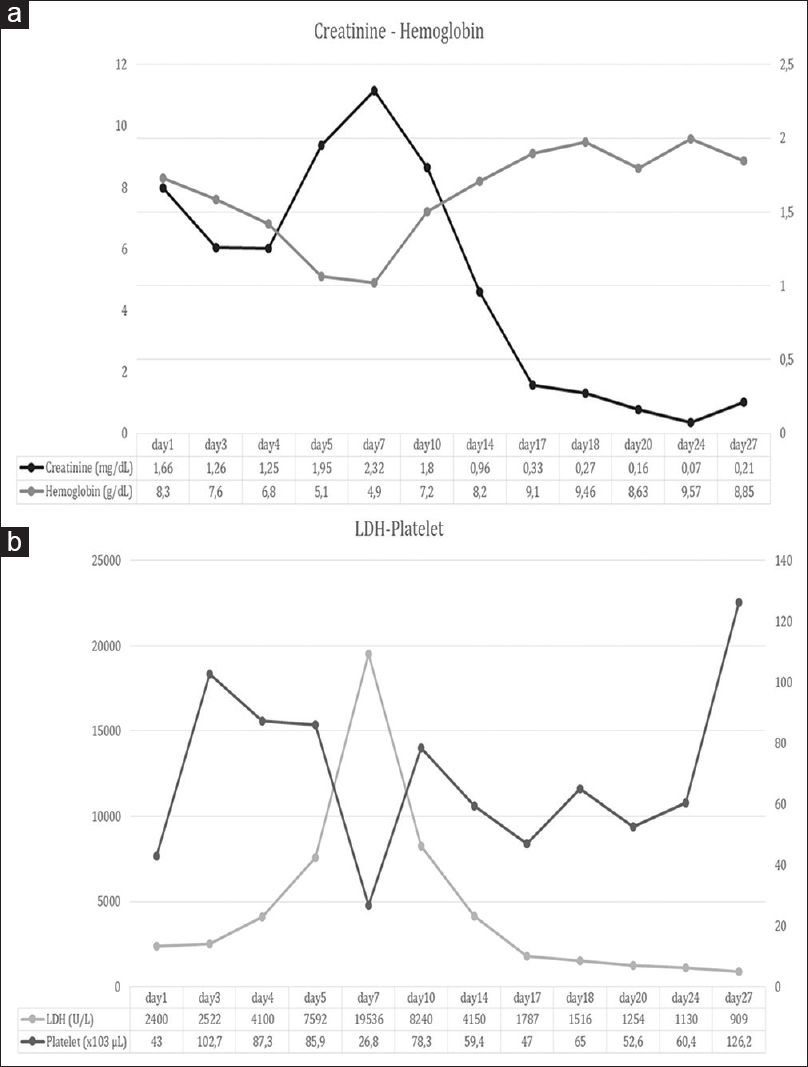
- Changes in hemoglobin and creatinine levels (a) and lactate dehydrogenase and platelet values (b) over time
Discussion
Diagnosing renal infiltration in children who have recently been diagnosed with acute leukemia is very challenging. Infections, nephrotoxic drugs, and TLS are other causes of acute kidney injury in such cases, and it can be difficult to distinguish which condition is responsible for observed renal damage.[1] As we observed in our case, bilateral renal enlargement, presence of blast cells in urine, and kidney dysfunction are strong predictors of leukemic infiltration of the kidney in our case.
aHUS is a rare but serious life-threatening complication in patients with renal infiltration of leukemia. When we searched the literature for aHUS in patients with ALL, we found only eight pediatric cases in which aHUS developed secondary to leukemic infiltration or chemotherapy.[2345678] Similarly, simultaneous aHUS and ALL have been previously reported in only one case who resolved with induction chemotherapy in a childhood series.[2] Although anemia, thrombocytopenia, and elevated LDH are common abnormalities in patients with leukemia, coexistence of the second unexplained LDH elevation with hemolytic anemia, thrombocytopenia, and renal dysfunction should alert the physician to the likelihood of aHUS development. In parallel with these findings, aHUS was detected in the 1st week of leukemia diagnosis in our case.
Early diagnosis and treatment of aHUS and underlying hematological problem are of critical importance for the patient's survival. In most of the published cases, aHUS resolved with initiation or discontinuation of chemotherapy depending on the etiology.[2345678] However, our case did not respond to steroid induction for renal infiltration complicated by aHUS. No standard approach for aHUS has been reported to date. The benefit of TPE in a recently published an international consensus approach for aHUS in children was uncertain.[10] However, TPE for 2 consecutive days produced marked reduction in serum LDH level and elevation Hb level, platelet count, and resolution of renal dysfunction in our case. Similar successful TPE administration was previously described in a 37-year-old Spanish male who developed renal failure with HUS secondary to acute promyelocytic leukemia.[11] It has been suggested that some chemokines release or cancer cell lines glycoprotein receptor overexpression resulting in platelet and fibrin formation in renal endothelial cell during the acute phase of leukemia may contribute to the development of aHUS in these cases.[12] TPE can be used to rapidly reduce these substances in such cases with aHUS secondary to leukemic infiltration of the kidney.[13]
Conclusion
It is emphasized that TPE should be kept in mind if there are laboratory findings of unexplained LDH elevation with microangiopathic hemolytic anemia, thrombocytopenia, and renal dysfunction supporting aHUS in patients with renal infiltration of leukemia at diagnosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Renal changes in acute leukemia in children at onset. Incidence and prognostic value. Pediatr Med Chir. 1982;4:107-13.
- [Google Scholar]
- Simultaneous occurrence of atypical hemolytic uremic syndrome and acute lymphoblastic leukemia: A case report and literature review. Pediatr Nephrol. 2008;23:835-9.
- [Google Scholar]
- Hemolytic uremic syndrome followed by acute lymphocytic leukemia. Int J Pediatr Nephrol. 1986;7:169-71.
- [Google Scholar]
- Hemolytic-uremic syndrome as a presenting form of acute lymphocytic leukemia. Ann Hematol. 2000;79:452-4.
- [Google Scholar]
- Acute leukemia: An association with atypical hemolytic uremic syndrome. Pediatr Nephrol. 2003;18:703-5.
- [Google Scholar]
- Hemolytic uremic syndrome secondary to the treatment of acute lymphoblastic leukemia. J Pediatr Hematol Oncol. 2000;22:483-4.
- [Google Scholar]
- Atypical haemolytic uraemic syndrome as a complication of induction chemotherapy for acute lymphoblastic leukaemia. J Clin Pathol. 2004;57:667-9.
- [Google Scholar]
- Hemolytic uremic syndrome in a child with leukemia and cytomegalovirus infection. Pediatr Nephrol. 2000;14:1118-20.
- [Google Scholar]
- Identification of renal infiltration based on urinary findings in a child with burkitt leukemia/lymphoma. Am J Hematol. 2017;92:839-40.
- [Google Scholar]
- An international consensus approach to the management of atypical hemolytic uremic syndrome in children. Pediatr Nephrol. 2016;31:15-39.
- [Google Scholar]
- Renal cortical necrosis secondary to thrombotic microangiopathy in the context of acute promyelocytic leukaemia blast crisis. Nefrologia. 2013;33:845-8.
- [Google Scholar]
- Role of tumor cell glycoproteins immunologically related to glycoproteins ib and IIb/IIIa in tumor cell-platelet and tumor cell-matrix interactions. FASEB J. 1988;2:2385-95.
- [Google Scholar]




