

Translate this page into:
Left Inferior Vena Cava from the Perspective of Laparoscopic Donor Surgeon: Anatomic Considerations and Surgical Implications
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Renal vascular aberrations are not uncommon cause for rejection of living kidney donors. While screening a donor for laparoscopic nephrectomy, we encountered a rare, yet important aberration in the form of left-sided inferior vena cava (IVC). There was an initial dilemma regarding the acceptability of the donor and which side kidney to select for donation. Scant literature is available on this particular clinical scenario, and only after a detailed study of the embryology and anatomy of IVC, were we able to make an informed choice. This article highlights the surgical anatomy and clinical implications of this rare condition from the perspective of laparoscopic donor surgeon.
Keywords
Donor nephrectomy
inferior vena cava
laparoscopy
vascular anomalies

Introduction
Left-sided inferior vena cava (LIVC) is a rare anatomic aberration and is found in only 0.17%–0.5% of the general population.[1] We encountered this anomaly on cross-sectional imaging in a prospective renal donor, who was planned to undergo laparoscopic donor nephrectomy (LDN). In the field of transplantation, availability of organs is scarce and rejecting an organ on account of a technical difficulty, anticipated due to abnormal anatomy, does not seem justified.
Left LDN is preferred over the right side, even in the presence of abnormal left renal vasculature, primarily because of longer renal vein, which facilitates anastomosis.[234] We initially considered the option of right LDN, in this case, as we presumed that since the IVC is left sided, the right renal vein would be longer, but after the review of LIVC anatomy and a detailed review of computed tomography (CT) angiogram, along with a radiologist, we realized that nothing could be farther from the truth. In this case, literature is scant and a detailed embryologic and anatomic knowledge of the IVC is necessary to make an informed decision and avoid catastrophic complications.[5]
Case Report
The prospective kidney donor was a 60-year-old mother, who was planned for left LDN. Her preoperative CT renal angiogram reported left renal vein of 29 mm and right renal vein of 23 mm with bilateral, single renal arteries. There was no mention of any vascular aberration on the CT angiogram report. In our unit, it is a routine practice to review the angiography films on radiology console, preferably with the radiology colleague, before surgery. During this session, LIVC was noted which actually was missed by the reporting radiologist [Figure 1].
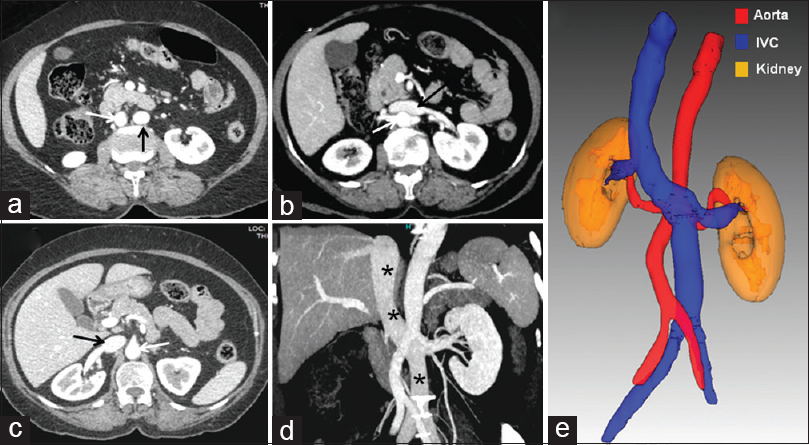
- Left-sided inferior vena cava. Axial contrast-enhanced computed tomography images from caudal to cranial (a-c) show the left-sided inferior vena cava crossing the midline from left to right of the aorta anteriorly at the level of left renal vein and then united with right renal vein to form a normal right-sided suprarenal inferior vena cava (inferior vena cava - black arrows; aorta - white arrows). Maximum intensity reformatted coronal image (d) and volume-rendered image (e) further confirm the left-sided inferior vena cava crossing from left to right (black asterisk in d)
Transperitoneal left LDN was performed as per the standard procedure using four ports. Intraoperatively, IVC was found on the left side of aorta till left renal vein, where it crossed over the aorta to continue cranially on the right side [Figure 2]. The origin of left renal artery was retrocaval. Using gentle upward traction on the kidney with left-hand instrument, left renal vein was clipped along with a cuff of IVC using two 15 mm Hem-o-lok clips (Weck Closure Systems, Research Triangle Park, NC, USA). The kidney was extracted using Pfannenstiel incision. There were no intraoperative issues, and the surgery was accomplished as any other left LDN. The measured length of graft renal vein was about 23 mm and it was anastomosed without any difficulty to the recipient's right external iliac vein. Postoperative period was uneventful, and the donor was discharged on the third postoperative day. Recipient's recovery was also unremarkable.
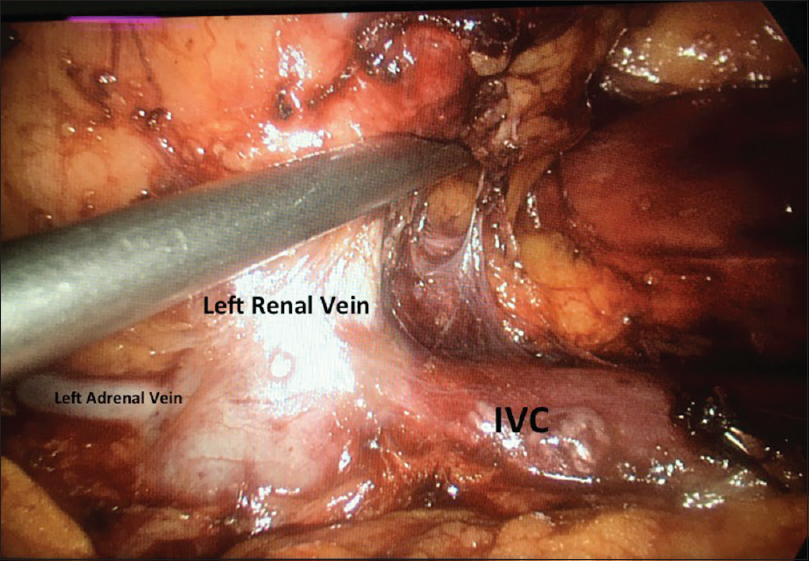
- Intraoperative image showing left renal hilar anatomy. Left renal vein is shorter in length, joining inferior vena cava which is present on the left side of aorta. Left adrenal vein is draining directly into inferior vena cava, while left gonadal vein is draining into left renal vein (lifted by left hand working instrument). Left renal artery is retrocaval (not seen)
Discussion
The IVC is formed as a result of selective emergence and regression of the cardinal, subcardinal, and supracardinal veins. In the initial embryological stages, the paired anterior and posterior cardinal veins drain the cephalic part and rest of the embryo, respectively. The cardinal veins form a symmetric system by the 4th week of gestation, and thus, potentially the adult IVC can lie on either side depending on which of these fetal veins regress. The posterior and supracardinal veins are dorsal, and the subcardinal vein is ventral. For the adult IVC to form, these two symmetrical systems must anastomose so that blood drains from left to right. The left subcardinal vein regresses and the right subcardinal vein persists as the renal segment of the IVC. Similarly, the left supracardinal vein and the lumbar portion of the posterior cardinal veins regress. Thus, the right supracardinal vein forms the definitive IVC just below the junction of the renal veins and IVC [Figure 3]. Now, if the left supracardinal vein does not disappear, a duplicate IVC is formed. In addition, if the right supracardinal vein regresses, a LIVC results. Hence, LIVC results from the left supracardinal vein and right subcardinal vein. Thus, from caudal to cranial, it is seen as lying ventral to the aorta, and after receiving the left renal vein, it crosses anterior to the aorta to reach its normal position on the right side [Figures 1e and 4].[6] The origin of the right renal vein is normal. This anatomic fact has important clinical relevance for laparoscopic donor surgeon.

- Diagrammatic representation of developmental anatomy of inferior vena cava. (a) initial stages (b) later stages of development with regression of rudimentary parts of the vein

- The artistic impression of the anatomy of left inferior vena cava
Conventionally, left-sided LDN is preferred based on the fact that the left renal vein is much longer than the right renal vein, which aids anastomosis and has easier surgical approach. The presumption that, in a case of LIVC, the entire IVC is on the left side (i.e., there is exact reversal of anatomy) and right renal vein is longer as compared to left and has the same configuration as left renal vein in normal individuals, and right LDN will be technically easier, is wrong.
The mere presence of a LIVC should not be a contraindication to LDN. Simforoosh et al.[5] and Radolinski et al.[7] reported the feasibility and safety of LDN in LIVC. Simforoosh et al., in their series of three incidentally detected LIVC intraoperatively, observed that it does not impact the outcome of elective LDN. However, we find CT angiograms to be important in detecting any vascular aberration preoperatively and suggest that the surgical team should themselves review the renal angiograms before surgery (preferably over console) rather than reviewing the reports or even films, to avoid any intraoperative surprises. The radiology report, at times, does not mention all the anomalies that are not considered important from a radiologist's perspective. However, they may be important from a clinician's perspective, like in the present case. Therefore, we suggest that a radiologist should be a part of the multidisciplinary team to evaluate all potential donors preoperatively. Implementation of the WHO surgical safety checklist in day-to-day practice is strongly recommended for improving patient outcomes.
In a LIVC, both the renal veins are shorter in length. Simforoosh et al. also found it interesting that in spite of a short left renal vein stump (~1.5 cm), its anastomosis was easier compared to right renal vein. In our case, we could achieve left renal vein stump of about 23 mm and it was anastomosed without any difficulty. Thus, in a case of LIVC, it is not mandatory to choose right kidney over left for donation.
Radolinski et al.[7] and Simforoosh et al.[5] used an Endo GIA stapler and two Hem-O-Lok clips, respectively, for renal vein clipping. We achieved an adequate left renal vein by applying two Hem-O-Lok clips, one below and one above the level of adrenal vein [Figure 2], which is a routine for our all LDNs.
Conclusion
LIVC is not a contraindication for LDN. The anatomy of LIVC is such that it is not an exact reversal of the normal anatomy, thereby the assumption that right renal vein will be longer, akin to left renal venous anatomy in normal individual, may not be correct. Every donor surgeon should be aware of this anatomic fact. Hence, these patients do not have the advantage of left long renal vein, and still left LDN is safe and feasible, provided the multidisciplinary team has reviewed the angiography images in detail and knows the presence of this anomaly beforehand.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Mr. Aman Anand for contributing Figures 3 and 4.
References
- Gonz conflicts of interest. ipa IS, Alarcz conflicts of interest. ided Inferior vena cava and aortoiliac surgery. Eur J Vasc Endovasc Surg Extra. 2008;5:9-11.
- [Google Scholar]
- Should the indications for laparascopic live donor nephrectomy of the right kidney be the same as for the open procedure? Anomalous left renal vasculature is not a contraindiction to laparoscopic left donor nephrectomy. Transplantation. 2001;71:660-4.
- [Google Scholar]
- Kidney transplants from living related donors having double inferior vena cava. Urol Int. 2004;72:358-60.
- [Google Scholar]
- Laparoscopic nephrectomy in patients with renal vein and/or inferior vena cava anomalies: Video presentation. Int J Urol. 2009;16:854.
- [Google Scholar]
- Left-sided inferior vena cava found incidentally during laparoscopic donor nephrectomy: Report of three cases. J Endourol. 2007;21:542-4.
- [Google Scholar]
- Langman's Medical Embryology. (13th ed). Philadelphia: Wolters Kluwer; 2015. p. :210-1.
- [Google Scholar]




