

Translate this page into:
Takotsubo Syndrome during Haemodialysis
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Takotsubo syndrome (TS) is typically characterized by transient (reversible) systolic dysfunction of the apical and mid segments of the left ventricle (LV), usually without obstruction of coronary arteries, in postmenopausal women after a stressful event. Usually, patients may experience symptoms such as chest pain, shortness of breath, palpitations, and rarely syncope or cardiogenic shock. There are many theories about pathophysiology of TS. Among these, most acceptable is the catecholamine theory. The prognosis is usually good with recovery of symptoms and imaging findings at most within a few weeks. However, complications may occur. We present the 11th published case of a patient on hemodialysis, who presented with TS and discuss why this situation may occur in patients on hemodialysis. Contrary to our patient, half of previously published cases presented with atypical symptoms. Therefore, it is important to be alert in order to timely diagnose, support the patient, and treat if any complications appear.
Keywords
Broken heart syndrome
hemodialysis
takotsubo syndrome

Introduction
Takotsubo syndrome (TS) is typically characterized by transient (reversible) systolic dysfunction of the apical and mid segments of the left ventricle (LV), usually without obstruction of coronary arteries, in postmenopausal women after a stressful event.[1234] It is also known as left ventricular apical ballooning syndrome, broken heart syndrome, or stress-induced cardiomyopathy. TS was first described in Japan in 1990 and owes its name to ancient Japanese traps for octopus.[5] The number of cases of TS reported is now relatively high probably because of the increased alertness of the medical staff.[3] There are many theories about pathophysiology of TS but among them more prevalent is the catecholamine theory, which can explain the appearance of TS in end-stage renal disease patients. In this case report, we present the 11th case of a patient on hemodialysis, who presented with TS and complicated with cardiogenic shock, which is a very rare complication of the syndrome and restored in few days.[6]
Case Report
A 55-year-old female patient with past medical history of end-stage renal disease on hemodialysis for 2 years because of rapidly progressive crescentic glomerulonephritis, vasculitis and inflammatory bowel disease, presented with chest pain and substernal heaviness during hemodialysis treatment. On presentation, the blood pressure was 140/80 mmHg, heart rate of 100/min, and respiratory rate of 15/min. The electrocardiogram showed Q waves in V1--V3 precordial leads, slight ST elevations in V1--V5 (1--2 mm), and inverted T waves in I, II, avL, avF, V4--V6 [Figure 1]. The echocardiogram revealed akinesia of middle and apical myocardial segments with hyperkinesis of the basal segments and severe systolic dysfunction (LV ejection fraction = 15%). She was treated as an acute coronary syndrome with dual loading antiplatelet therapy with aspirin and clopidogrel, transferred to the catheterization laboratory and submitted to coronary angiogram. The latter showed coronary arteries with no significant obstruction [Figure 2] and slow flow. The cardiac enzymes were elevated: High sensitive cardiac troponin = 12.500 ng/L (normal values: 0--15.6 ng/L) and CPK/CKMB = 1180/90 IU/L (normal values: CK = 0--220 IU/L and CKMB: 0--23 IU/L). She was diagnosed with Takotsubo cardiomyopathy. Two hours after the coronary angiogram patient presented with cardiogenic shock with hypotension (blood pressure = 85/50 mmHg), acute pulmonary edema, and abdominal pain. She was submitted to emergent hemodialysis after excluding mesenteric ischemia with an abdominal computed tomography. The patient's condition slowly improved. Twenty-four hours later, the blood pressure was normal, the patient was not dyspneic and asymptomatic. A new echocardiography 5 days afterwards showed persistent severe systolic dysfunction of the LV and also revealed a sizeable thrombus in the middle and apical anterior segments of the LV [Figure 3]. Acenocoumarol was added to her medications. Ten days after the acute presentation, the LV systolic function had normalized and the patient was discharged with dual antiplatetet therapy (aspirin-clopidogrel), acenocoumarol, bisoprolol, enalapril, omeprazole, and her previous medications for renal disease (sevelamer, paricalcitol). During the echocardiography after a month follow-up, the thrombus was absent [Figure 4]. The patient discontinued dual antiplatelet therapy and after 3 months discontinued acenocoumarol. This is the 11th case of Takotsubo cardiomyopathy presented in a patient on hemodialysis, complicated with cardiogenic shock and apical thrombus formation.
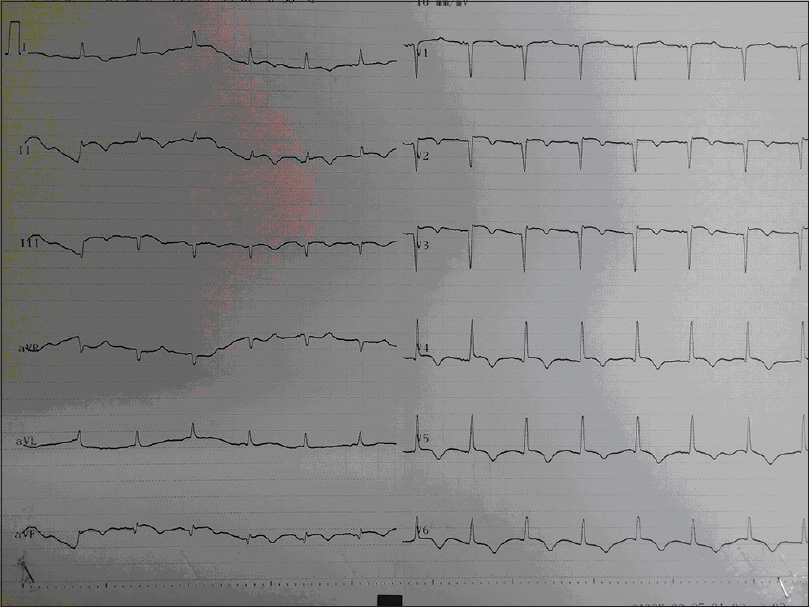
- ECG during the acute phase

- Coronary angiogram showed no obstructed coronary arteries

- A sizeable thrombus appeared in the echocardiography, five days after the acute presentation

- One month after the acute presentation and after taking acenocoumarol, the thrombus was solved
Discussion
Demograhics, stressors and pathophysiology of TS
Takotsubo syndrome has mainly female predominance, typically postmenopausal women.[178] It is often associated with a stressful event (emotional or physical). TS can be categorized in two clinical subtypes: primary (without clearly identifiable stressor trigger) and secondary (due to specific triggers).[38910] There are many theories about pathophysiology of TS. These include catecholamine theory, myocardial bridging and myocardial edema, microvascular dysfunction, hormonal and genetic factors, theory for the role of hypovolemia, hyponatremia and syndrome of inappropiate hypersecretion of ADH (SIADH), mechanic hypothesis (according to which anatomic variants of the sympathetic nervous system and the distribution of adrenoreceptors are responsible for the expression of TS), and theories about the role of carbohydrate antigen 125 and interleukins 6 and 10.[78] Among these, most acceptable is the catecholamine theory,[9] according to which the excessive release of catecholamines or their exogenous administration is related to the occurrence of the syndrome as catecholamines change β-adrenergic receptor signalling and particularly induce β2-coupling from Gs to Gi. Epinephrine in low and medium doses acts as a positive inotropic agent but in high doses acts as a negative inotropic agent because it is causing β2-coupling from Gs (stimulatory) to Gi (inhibitory). The resulting decline of myocyte contractile function is evidenced by echocardiography. The area most affected is the apex because of the higher concentration of adrenoreceptors.[37811]
Some authors have previously thought that TS appears in the context of myocardial stunning seen in these patients.[12] However, recent articles differentiate the two entities. More specifically, myocardial stunning usually occurs with a clinical picture of acute heart failure, negative T on the electrocardiogram, and akinesia/hypokinesia of basal and middle myocardial segments in the echocardiogram. Conversely, TS appears usually with clinical picture of acute coronary syndrome, ST elevation in the electrocardiogram, and akinesia/hypokinesia of medial and apical myocardial segments. Myocardial stunning may be ischemic or neurogenic and is characterized by transient LV dysfunction. Ischemic is observed after an acute coronary syndrome, whereas neurogenic is observed as part of the cardiorenal syndrome, due to reduced metabolic regulation of blood flow, calcium overload, microvascular dysfunction or inflammation.[1314]
The diagnosis of TS is important in order to offer the proper therapy.
Diagnosis of TS
From time to time, several diagnostic criteria for TS have been proposed with the most prevalent being the Mayo Clinic criteria and the Heart Failure Association diagnostic criteria. Currently, the criteria proposed by International Expert Consensus Document[4] on TS to be used are the following:
Patients show transient LV dysfunction (hypokinesia, akinesia, or dyskinesia) presenting as apical ballooning or mid ventricular, basal, or focal wall motion abnormalities. Right ventricular involvement can be present. Besides these regional wall motion patterns, transitions between all types can exist. The regional wall motion abnormality usually extends beyond a single epicardial vascular distribution; however, rare cases can exist where the regional wall motion abnormality is present in the subtended myocardial territory of a single coronary artery (focal TTS)
An emotional, physical, or combined trigger can precede the TS event, but this is not obligatory
Neurologic disorders (e.g., subarachnoid haemorrhage, stroke/transient ischaemic attack, or seizures) as well as pheochromocytoma may serve as triggers for TS
New ECG abnormalities are present (ST-segment elevation, ST-segment depression, T-wave inversion, and QTc prolongation); however, rare cases exist without any ECG changes
Levels of cardiac biomarkers (troponin and creatine kinase) are moderately elevated in most cases; significant elevation of brain natriuretic peptide is common
Significant coronary artery disease is not a contradiction in TS
Patients have no evidence of infectious myocarditis
Postmenopausal women are predominantly affected.
As can be seen from the diagnostic criteria mentioned above, there are many parameters that should be considered for the diagnosis of TS.
Clinical presentation
Usually, patients may experience symptoms such as chest pain, shortness of breath, palpitations, and rarely syncope or cardiogenic shock. Rarely, they may be completely asymptomatic and the diagnosis based on the echocardiographic study. The above picture usually occurs after a stressor trigger.[189]
Biomarkers
Cardiac troponin is elevated in >90% of patients with TS but is disproportionately low relative to the extent of dysfunctional myocardium. Instead, the BNP or/and NT-proBNP levels are correlated more closely with the severity of ventricular wall motion abnormalities.[178910]
Electrocardiography findings
The ECG findings may include: ST-segment elevation, ST-segment depression, new LBBB, Q waves, widespread T-wave inversion, and significant QT prolongation (the latter predisposes to torsades de pointes and ventricular fibrillation).[1789]
Imaging
Echocardiography usually reveals transient regional wall motion abnormalities (hypokinesis, akinesis, or dyskinesis) and reduced LV ejection fraction. Sometimes mitral regurgitation can be observed due to the systolic anterior mitral leaflet movement and obstruction of the LV outflow tract (LVOT). Echocardiography also may reveal apical thrombus, which is a potential cause of emboli.
The classical pattern in left ventriculography includes wall motion abnormalities of the apical and mid ventricular segments, extending beyond the distribution of a single epicardial coronary. Less common patterns include mid ventricular pattern in which apical function is preserved and inverted/reverse pattern in which mid- and apical segments are preserved with akinesis/hypokinesis of the basal regions.[189]
Although unobstructed coronary arteries was a prerequisite in the previous diagnostic criteria, in the last proposed criteria[4] it is clarified that the presence of coronary disease does not reject TS diagnosis and should be evaluated taking account the regional wall motion abnormalities that correspond or not to the territory of the involved coronary artery.
Cardiac magnetic resonance imaging can reveal transient wall motion abnormalities without late gadolinium enhancement.[78910]
Management and prognosis
The prognosis is usually good with recovery of symptoms and imaging findings at most within a few weeks.[5810] However, complications may occur such as acute heart failure, LVOT obstruction, mitral regurgitation, cardiogenic shock, arrythmias, thrombus formation, pericardial effusion, ventricular wall rupture, and right ventricular involvement, which need appropriate treatment.[89] Yassin et al.[15] studied that the patients with TS and advanced chronic kidney disease had worse prognosis in comparison to patients with less advanced chronic kidney disease, and concluded that there was difference in prognosis concerning the possibility of acute kidney injury and duration of hospitalization but no difference in mortality. Treatment is personalized to each patient depending on whether they have low- or high-risk characteristics and is usually supportive. In rare cases, therapy may include during the acute phase: intra-aortic baloon pump, ventilatory support, and continuous veno-venous hemofiltration in hemodynamically unstable patients. Drugs that stimulate the sympathetic system should be avoided. In LVOT obstruction, b-blockers are recommended. Hemodynamically stable patients are treated with b-blockers, diuretics, and angiotensin-converting enzyme inhibitors. For thrombus formation in LV, anticoagulation treatment is also indicated. Of course, secondary TS also involves treating the original cause.[37891011]
TS in end-stage renal disease
Patients with end-stage renal disease are thought to have increased activity of the sympathetic system,[16] and therefore high levels of circulating catecholamines. This state of sympathetic overactivity may be one of the causes of the high risk of arrhythmias and sudden cardiac death in which these patients are exposed. This pathophysiologic substrate combined with mental stress and depressive mood disorders, which are often present in these patients, may be the precipitating factors for TC.[25] According to another theory, TS is caused by oxidative stress. More specifically, hemodialysis leads to loss of antioxidant factors and causes disturbance in the balance between oxidative and antioxidant factors resulting in the influence of the contractibility of the heart.[17] Also in hemodialysis, patients often coexist anemia, poor nutrition, muscle weakness, associated diabetes mellitus, volume overload, and other comorbidities that lead to poor quality of life and increased physical and emotional stress, which are substrate for TS.[518] The case we present is the 11th case of a patient on hemodialysis who presented TS. Contrary to our patient, half of all these published cases presented with atypical symptoms. Therefore, it is important to be alert in order to timely diagnose, support the patient, and treat if any complications appear.
Conclusion
It is clear that TS is an important entity and although its diagnosis may be delayed due to atypical symptoms, it usually has a good prognosis. TS, as we explained, may occur for various reasons also in hemodialysis patients. Further research is needed in order to clarify the underlying mechanism. This will help to reduce the incidence of TS, which may sometimes have serious complications, as in the case of our patient.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Broken heart syndrome in a patient on maintenance hemodialysis. J Investig Med High Impact Case Rep 2017:5. doi: 10.1177/2324709617713512
- [Google Scholar]
- Epidemiology, pathogenesis, and management of takotsubo syndrome. Clin Auton Res. 2018;28:53-65.
- [Google Scholar]
- International expert consensus document on takotsubo syndrome (Part I): Clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J. 2018;39:2032-46.
- [Google Scholar]
- Takotsubo cardiomyopathy in two patients without any cardiac symptom on maintenance hemodialysis. Case Rep Nephrol. 2013;2013:640976.
- [Google Scholar]
- Takotsubo syndrome and dialysis: An uncommon association? J Int Med Res. 2018;46:4399-4406.
- [Google Scholar]
- Takotsubo cardiomyopathy: Pathophysiology, diagnosis and treatment. World J Cardiol. 2014;6:602-9.
- [Google Scholar]
- Current state of knowledge on takotsubo syndrome: A position statement from the taskforce on takotsubo syndrome of the heart failure association of the european society of cardiology. Eur J Heart Fail. 2016;18:8-27.
- [Google Scholar]
- Pathophysiology of takotsubo syndrome: Temporal phases of cardiovascular responses to extreme stress. Circ J. 2014;78:1550-8.
- [Google Scholar]
- Neurogenic stunned myocardium vs. takotsubo syndrome: We should stop making a distinction. Int J Cardiol. 2014;177:166.
- [Google Scholar]
- Are there differences between takotsubo cardiomyopathy and neurogenic stunned myocardium? A prospective observational study. Int J Cardiol. 2014;177:1108-10.
- [Google Scholar]
- Takotsubo cardiomyopathy and neurogenic stunned myocardium: Similar albeit different. Eur Heart J. 2016;37:2830-2.
- [Google Scholar]
- Clinical impact of advanced chronic kidney disease on outcomes and in-hospital complications of takotsubo syndrome (broken-heart-syndrome): Propensity-matched national study. Int J Cardiol 2018:pii: S0167-5273 (18) 35026-5. doi: 10.1016/j.ijcard. 2018.09.098. [Epub ahead of print]
- [Google Scholar]
- Increased sympathetic renal innervation in hemodialysis patients is the anatomical substrate of sympathetic hyperactivity in end-stage renal disease. J Am Heart Assoc 2015:4. doi: 10.1161/JAHA.115.002426
- [Google Scholar]
- Clinical features of patients with stress-induced cardiomyopathy associated with renal dysfunction: 7 case series in single center. BMC Nephrol. 2013;14:213.
- [Google Scholar]
- 'Takotsubo' cardiomyopathy in a maintenance hemodialysis patient. Ther Apher Dial. 2006;10:94-100.
- [Google Scholar]




