

Translate this page into:
Bilateral Perinephric Collections in Nephrotic Syndrome
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 21-year-old lady, with history of childhood nephrotic syndrome was referred with a relapse. Ultrasound abdomen and non-contrast computed tomography (NCCT) showed bilateral massive renal subcapsular collections [Figures 1 and 2]. Duplex imaging confirmed normal flow across the renal vessels. A lymphangioscintigraphy showed normal lymphatic flow. A technetium 99 labelled L, L-ethylenedicysteine (LLEC) scan showed normal parenchymal function and non-obstructed drainage in both kidneys. An ultrasound-guided aspiration of the perinephric fluid revealed a transudate (no cells, protein 0.7 gm/dL; albumin 0.2 gm/dL). Since the patient had a history of steroid-responsive nephrotic syndrome, she was restarted on prednisolone 1 mg/kg/day, assuming that remission of nephrotic state would lead to the resorption of the perirenal fluid collections. A repeat ultrasound was done after one and a half months of attaining a complete remission. It showed persistent fluid collections, with similar dimensions prior to the start of steroid therapy. Hence, a laparoscopic fenestration of Gerota's fascia was performed on the left side, along with a kidney biopsy. The renal capsule was considerably thicker and had a fibrous texture. Biopsy from the renal capsule showed fibro-adipose and fibro collagenous tissue admixed with plasma cells and lymphocytes. We did not drain the right side, assuming that it might resolve in due course. The kidney biopsy was suggestive of Focal Segmental Glomerulosclerosis––not otherwise specified. We reassessed the patient at the end of three months, which showed persistent perinephric collections on the right side. A fenestration procedure was done on the right side as well. Her steroids were stopped after 4 months. She continues to be in remission, with no recurrence of subcapsular fluid collection.
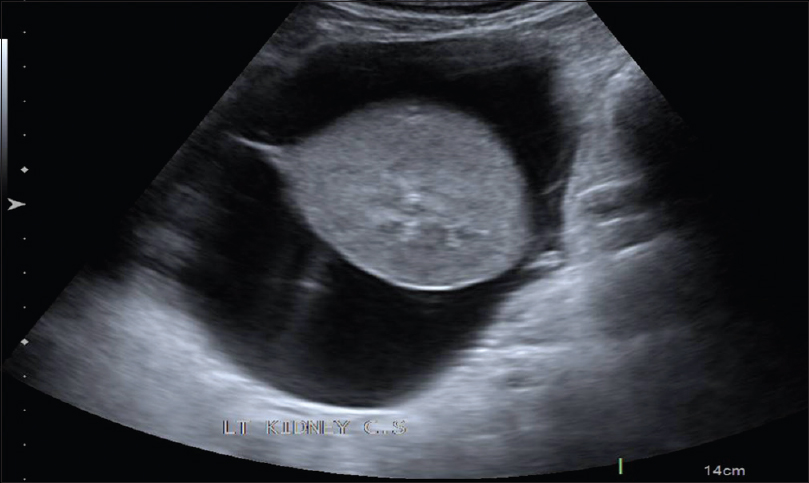
- Ultrasound abdomen of left kidney showing subcapsular fluid collections

- Plain CT abdomen showing massive perinephric collections
Renal subcapsular fluid collections are due to the accumulation of blood, pus, or urine postoperatively. Subcapsular transudate collections were reported in about 14% of cases with chronic kidney disease.[1] There are only a few reports of subcapsular fluid collections in patients with Nephrotic syndrome. The exact pathophysiology is not known. The renal subcapsular fluid collections have been reported in membranoproliferative glomerulonephritis, focal segmental glomerulosclerosis, lupus nephritis, amyloidosis, and in membranous nephropathy with renal vein thrombosis.[2345] The potential pathophysiologic mechanisms include renal vein thrombosis, leading to increased hydrostatic pressure. In the presence of significant hypoalbuminemia associated with the nephrotic syndrome, this would lead to extravasation of fluid into the subcapsular spaces. An alternative hypothesis proposed is excessive sodium retention leading to the formation of sub-capsular fluid collections.[12] There are case reports of successful management through percutaneous pigtail catheter drainage[3] or fenestration of Gerota's fascia.[4] There are reports of continuous fluid drainage from the percutaneous drain, requiring the instillation of povidone-iodine.[5] There are no recurrences reported after the fenestration of Gerota's fascia. With a background history of prolonged nephrotic state, considering the possibility that the drain might never become dry, we have opted for laparoscopic fenestration and drainage of fluid into the peritoneal cavity.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Perirenal lucency (“kidney sweat”): A new sign of renal failure. Am J Roentgenol. 1999;173:1075-7.
- [Google Scholar]
- Perirenal fluid in renal parenchymal medical disease ('floating kidney'): Clinical significance and sonographic grading. Clin Radiol. 2001;56:979-83.
- [Google Scholar]
- Fenestration of the Gerota's fascia as symptomatic treatment of floating kidneys. Am J Kidney Dis. 2007;50:1020-2.
- [Google Scholar]
- Perirenal subcapsular fluid collection in a patient with membranous nephropathy and renal vein thrombosis. J Urol. 1986;136:1287-9.
- [Google Scholar]




