

Translate this page into:
Arterial Thrombosis Associated with Factor V Leiden Mutation in a Child with Nephrotic Syndrome
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Thromboembolism remains a common complication of nephrotic syndrome (NS) in adults and a less common complication in children. Venous thrombosis is well recognized, but arterial thrombosis occurs less frequently and is seen primarily in children. We report a case of arterial thrombosis associated with factor V Leiden (FVL) mutation in a young girl with NS. Screening for inherited thrombophilias such as FVL mutation may be beneficial for NS patients with thromboembolic vascular events not explained by conventional risk factors.
Keywords
Arterial thrombosis
factor V leiden mutation
nephrotic syndrome

Introduction
Among the complications of nephrotic syndrome (NS), thromboembolism is considered to be the most significant and life threatening after infections. Addis first reported thrombosis in patients with NS in 1948.[1] Thromboembolism remains a common complication of NS in adults (25%) and a less common complication in children (3%).[2] Venous thrombosis is well recognized, but arterial thrombosis occurs less frequently and is seen primarily in children.[3] The numerous abnormalities of the coagulation and homeostasis system in nephrotic patients may arise through distinct mechanisms: urinary loss of antithrombin III, platelet hyperactivity, thrombocytosis, alterations in the fibrinolytic system, and increased synthesis of procoagulant proteins.[4] Factor V Leiden (FVL) mutation has been reported as the most common hereditary cause of venous thrombosis.[56] Thirty to 60% of cases of familial thrombophilia and 3% to 7% of healthy people were found to have FVL mutation.[7] The risk of recurrent thromboembolic events is significantly higher in carriers of FVL mutation than in patients without this abnormality.[8] We report a case of arterial thrombosis associated with FVL mutation in a young girl with NS.
Case Report
A 12-year-old girl presented elsewhere in July 2015 with pain in right leg associated with bluish discoloration of all toes. On evaluation, she was found to have right popliteal artery thrombosis on doppler, which was treated with intraarterial catheter-guided thrombolysis, followed by transfemoral thrombectomy. In view of failure to salvage the limb, right above knee amputation was done. She was incidentally detected to have nephrotic proteinuria (urine spot PCR- 8.2), complete urine examination showed 4+ albumin, 30-35 RBC and 8-10 pus cells, and ANA was positive. She was given three doses of methyl prednisolone injection 1 g over 3 days and referred to our hospital for further treatment. She developed seizures and MRI brain was suggestive of acute infarct in right frontal lobe. She was started on prednisolone, levetiracetam, antiplatelets, statins and biopsy was deferred. She was on regular follow-up and in view of exacerbation of edema and proteinuria in March 2016, work-up was done for hypercoagulable state and she underwent renal biopsy.
Laboratory study showed urine -3+ albumin, 30--35 RBC, and 6--8 pus cells; 24-hour urine protein was 3 g; hemoglobin was 10.3 g/dl, white blood cells were 18,800/mm3, and platelet count was 290,000/mm3. Blood urea, creatinine, glucose, electrolytes, prothrombin, and partial thromboplastin times were within normal limits. Biochemical analyses revealed total protein 4 g/dl, serum albumin 2.3 g/dl, total cholesterol 280 mg/dl, C3-78 mg/dl, and C4-19 mg/dl. ANA (IF) showed 4+ homogenous pattern. Test results for anti-dsDNA, p-ANCA, c-ANCA, and anticardiolipin antibody were negative. Protein S was 73% (normal 57--113%), protein C 94% (normal 70–140%), and anti-thrombin III (AT III) 96% (normal 83–128%). Her homocysteine level was 47.3 μmol/L, B12-137 pg/ml, and folate levels-3.2 ng/ml. Finally, genetic study showed the heterozygous mutation for FVL (FV/G1691A) and normal for factor II variant.
Renal biopsy showed six glomeruli with endocapillary proliferation, normal thickness of glomerular basement membrane, and cellular crescent in one glomerulus. Tubules were closely paced, vessels and interstitium were unremarkable. IF showed peripheral coarse granular deposits of IgG and C3 in basement membrane [Figure 1]. These findings were suggestive of diffuse proliferative glomerulonephritis. She was treated with steroids and azathioprine and achieved sustained remission.
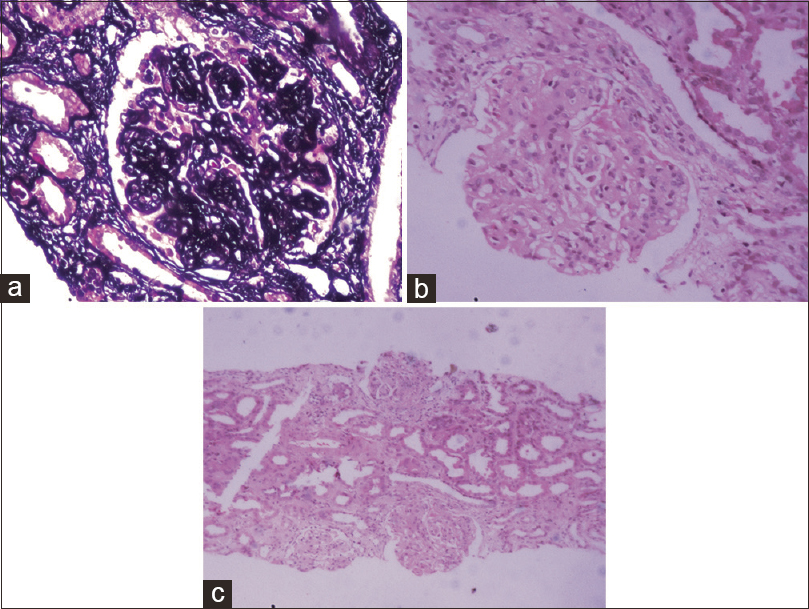
- 400×, SM stain, normal thickness basement membrane. 400×, H and E stain, glomerulus showing endocapillary capillary proliferation. 100×, H and E stain, Three glomeruli with endocapillary proliferation and normal tubules and interstitium
Discussion
The pathophysiology of thrombosis in NS is multifactorial. The first factor is patient's underlying genetic predisposition, which may be unrelated to their renal disease but influences their likelihood of developing thromboembolism.[9] This includes the known mutations and single nucleotide polymorphisms associated with thrombophilia (e.g., congenital antithrombin deficiency or FVL mutation) as well as unknown ones. The likelihood of an individual exceeding the thrombotic threshold is determined by these genetic factors in combination with environmental and acquired thromboembolism risk factors (e.g., inflammation, medications, central venous catheters).[9]
A well-established genetic predisposition to venous thrombosis is a single-point mutation in the gene encoding coagulation factor V [G1691A or FVL], with an average seven-fold increased risk of thrombosis in heterozygote and a 50-fold to 100-fold increased risk of thrombosis in homozygotes.[10] Previous studies have reported FVL prevalence among populations of up to 10% among Europeans.[11] Resistance to activated protein C is considered to be a major risk factor for venous thromboembolism. Because of this resistance, there is poor response to the anticoagulant activity of activated protein C, which causes a predisposition for a hypercoagulable state. At least 90% of the cases with resistance to activated protein C can be explained by FVL mutation.
The tendency of nephrotic patients to develop thrombotic episodes has been attributed to a hypercoagulable state because of coagulation protein abnormalities, impaired fibrinolysis and increased platelet aggregation, venous stasis, hemoconcentration, increased blood viscosity, and possibly the administration of diuretics and steroids.[4] Although the two important risk factors for the development of venous thrombosis are blood stasis and hypercoagulability, risk factors for arterial thrombosis include arterial hypertension, hyperlipidemia, smoking, diabetes mellitus, and obesity.[12]
Venous and arterial thrombosis is high among adult nephrotic patients compared with children, particularly those with idiopathic MGN.[13] The incidence of thromboembolic events in children with NS has been reported to range from 1.8% to 5%.[13] Typically, thrombotic events complicating NS have been reported in children with congenital NS, minimal change disease, and focal segmental glomerulosclerosis.[11] Although the risk of thrombotic events in children with NS might be lower, the severity of thrombotic events was much greater than in adults, with some children needing surgical intervention.[1314] In nephrotic patients, arterial thrombosis has been reported in the aorta, mesenteric, axillary, femoral, ophthalmic, carotid, cerebral, renal, pulmonary, and coronary arteries.[3] Although thrombosis is most frequent in the early months, it can occur at any stage after the onset of NS.
Our patient has heterozygous FVL mutation and high-homocysteine levels (secondary to B12 and folate deficiency). These may be individually responsible for popliteal artery thrombosis, leading to gangrene of right foot requiring amputation. Although Fabri et al.[15] suggested that inherited thrombophilia is not a strong risk factor for the development of nonrecurrent thrombosis in children with NS, a combination of mutation responsible for vascular event and NS is the most reliable cause of the arterial thromboembolism in our patient.
The number of anomalies and the intensity of alterations, which are responsible for thrombophilia seen in NS, vary from one patient to another and during flare-ups in the same patient. Today, it is understood that the coexistence of several factors is necessary to induce thromboembolic complication in these patients. The coexistence of FVL mutation and other coagulation abnormalities encountered in NS may facilitate thromboembolic complications.
Conclusion
Screening for inherited thrombophilias such as FVL mutation may be required for NS patients with thromboembolic vascular events not explained by conventional risk factors.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Glomerular Nephritis, Diagnosis and Treatment. Vol 1. New York: McMillan; 1948.
- Epidemiology and pathophysiology of nephrotic syndrome–associated thromboembolic disease. Clin J Am Soc Nephrol. 2012;7:513-20.
- [Google Scholar]
- Coagulation and thromboembolic complications in the nephrotic syndrome. Adv Nephrol. 1984;13:75-114.
- [Google Scholar]
- Hypercoagulability, renal vein thrombosis, and other thromboembolic complications of nephrotic syndrome. Kidney Int. 1985;28:429-39.
- [Google Scholar]
- Inherited thrombophilia: Resistance to activated protein C as a pathogenetic factor of venous thromboembolism. Blood. 1995;85:607-14.
- [Google Scholar]
- Association of idiopathic venous thromboembolism with single point-mutation of Arg506 of factor V. Lancet. 1994;343:1535-6.
- [Google Scholar]
- Venous thrombosis due to poor anticoagulantresponse to activated protein C: Leiden thrombophilia study. Lancet. 1993;342:1503-6.
- [Google Scholar]
- Inherited thrombophilia is associated with deep vein thrombosis in a Colombian population. Am J Hematol. 2006;81:933-7.
- [Google Scholar]
- Risk factors for venous thrombosis-current understanding from an epidemiological point of view. Br J Haematol. 2010;149:824-33.
- [Google Scholar]
- Mutation in blood coagulation factor V associated with resistance to activated protein C. Nature. 1994;369:46-67.
- [Google Scholar]
- Thrombotic complications in childhood-onset idiopathic membranous nephropathy. PediatrNephrol. 2003;18:1298-300.
- [Google Scholar]
- A case of deep vein thrombosis in idiopathic nephrotic syndrome with resistance to activated protein C. J Nephrol. 1998;11:76-7.
- [Google Scholar]
- Inherited risk factors for thrombophilia in children with nephrotic syndrome. Eur J Pediatr. 1998;157:939-42.
- [Google Scholar]




