

Translate this page into:
Role of Endovascular Treatment in Dysfunctional Hemodialysis Fistulae: A Single Center Experience
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Arteriovenous fistulas (AVFs) are the preferred route of hemodialysis in end-stage renal disease. However, recurrent patency loss is an obstacle in long-term maintenance. Endovascular treatments may provide a durable option for prolongation of patency in AVFs.
Methods:
Retrospective observational study was done on 46 patients with AVF for hemodialysis in the Department of Diagnostic and Interventional Radiology for a period of 1 year from September 2020 to August 2021. The characters of dysfunctional fistulas and results of various interventional procedures were assessed for technical and clinical success rates. Short-term follow-up records of patients were assessed for post-intervention primary patency (PIPP) and post-intervention assisted primary patency (PIAPP) of various procedures.
Results:
The most successful outcomes post intervention were seen in radio-cephalic fistulas formed more than 1 year ago with juxta-anastomotic narrowing. The overall technical success rate was 89.13% with a PIPP of 78.26% and a PIAPP of 82.60% at 3 months. PTA had better technical success rates (88.23%) as compared to dysfunctional segments with thrombosis that underwent angioplasty and thromboaspiration (84.2%). Central venous stenosis undergoing PTA and stenting had a 100% success rate. At 3 months follow-up, PIPP was better among the angioplasty plus thromboaspiration group (73.7%), while PIAPP rate was better in the angioplasty subgroup at 82.35%.
Conclusion:
Endovascular intervention is the first-line treatment in dysfunctional AVFs attributable to the multitude of options available, all of which have comparable outcomes, high success rates, and notable short-term patency.
Keywords
Angioplasty
endovascular intervention
hemodialysis

Introduction
The incidence of chronic kidney disease (CKD) is on the rise throughout the world. A population-based study estimated an age-adjusted incidence rate of end-stage renal disease (ESRD) to be 232 per million in the Indian population.[1] ESRD patients can also be on conservative treatment such as peritoneal or hemodialysis before they undergo transplant. Out of these, hemodialysis is the safest and most acceptable method. Hemodialysis requires creating a vascular access, which can be done by arteriovenous fistulas (AVFs), arteriovenous grafts (AVGs), and tunneled or non-tunneled catheters.[2]
AVFs are the preferred route of hemodialysis as they have lower morbidity and better patency results. However, creating a long-term AVF access is a challenge as approximately 50% of fistulas lose patency during the course of treatment.[3] However, with the advancement of endovascular procedures, the patency of AVFs for hemodialysis can be prolonged by various procedures, including percutaneous transluminal angioplasty (PTA); thromboaspiration, and vascular stenting.[4]
The study aimed at evaluating the role of endovascular procedures in various types of fistula dysfunctions at various anatomical sites, their indications, efficacy, and short-term patency.
Materials and Methods
This was a retrospective observational study based on the results of various endovascular procedures carried out for dysfunctional endovascular fistulas in the Department of Radio-Diagnosis & Interventional Radiology of a tertiary hospital in the Himalayan foothills done for a period of 1 year from September 2020 to August 2021.
Inclusion criteria
Patients with previous functional hemodialysis fistulas which were naïve to interventional procedures were included in the study with the following features:
Suboptimal dialysis flow rates.
Difficult cannulation
Altered thrill
-
Hemodynamically significant stenosis with or without thrombosis on USG
Doppler evaluation.
Central venous stenosis (CVS) precluding effective dialysis.
Exclusion criteria
Failed to mature fistula/Virgin fistula
Fistula presenting within 1 month of creation
Infected fistula or overlying cellulitis
Aneurysm with impending rupture.
Study design
After due clearance from the institute's ethical committee (ECR/710/Inst/UK/2015/RR-21) with approval no. SGRR/IEC/09/21, this retrospective observational study was done on imaging and hospital-based data. A consent waiver was obtained as the patients had already undergone the required investigations for clinical requirements. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Two vascular interventional radiologists independently assessed and documented the characters of dysfunctional fistulas and the results of various interventional procedures. Follow-up data of patients post endovascular procedures was obtained from the records of Out Patient Department (OPD) of the Vascular and Interventional Radiology clinic for a period of 3 months post procedure. Technical and clinical success rates, post-intervention primary patency (PIPP), and post-intervention assisted primary patency (PIAPP) were documented for various endovascular procedures. Correlation of various anatomical characters of hemodialysis fistulas, types of dysfunctions, and their doppler characteristics with the results of the suitable endovascular treatments were assessed.
For the purpose of this study, the following definitions were accepted[567]:
Mature Arteriovenous fistula: A fistula suitable for use when the diameter of a vein is sufficient for successful two-needle cannulation.
Functional Fistula: A dialysis circuit that has a) a flow of >600 mL/min or the vein has a minimum diameter of 6 mm for AVF; b) does not exceed a depth of 0.6 cm; c) 6-cm venous segment available for cannulation; d) optimal dialysis rates.
Dysfunctional fistula: a) An arteriovenous access with an abnormal hemodynamic (>50% reduction in diameter) or clinically significant parameter (recirculation/high venous pressure/decreased blood flow/swollen limb/altered thrill), precluding effective dialysis.
Juxta-anastomotic segment: Artery/vein <2 cm from anastomosis and anastomotic segment.
Functionally significant stenosis: A reduction of 50% or more in the diameter along with hemodynamic or clinical abnormalities such as recirculation/decreased blood flow/swollen limb/prolonged bleeding/altered thrill/reduction in dialysis kinetics/inability to puncture to perform hemodialysis.
Technical/Anatomical Success: <30% residual diameter stenosis post treatment (ideally 0); while for thrombotic segments, resumption of flow along with <30% residual diameter stenosis.
Clinical Success: Improvement of clinical and hemodynamic parameters with the resumption of normal dialysis for at least one session after treatment and continuous palpable thrill.
Post-Intervention Primary Patency (PIPP): Uninterrupted patency after intervention until next access thrombosis or re-intervention.
Post-Intervention Assisted Primary Patency (PIAPP): Patency following intervention until access thrombosis or surgical intervention that excludes the treated lesion from the access circuit. Endovascular treatment of restenosis in previously treated access or a new arterial or venous stenosis/occlusion (excluding access thrombosis) are compatible with assisted primary patency.
Clinical Examination: On inspection, any limb edema or dilated vascular channels were observed. Any signs of infections or impending aneurysm rupture were also assessed. Juxta-anastomotic stenosis was demarked by an evident bounding pulse at the anastomotic site with a systolic thrill instead of a soft continuous thrill. Venous stenosis was seen as the collapsed segment between puncture sites and a faint thrill.
Doppler Evaluation: Doppler examinations were performed with high-frequency linear probes (5–14 MHz). The area of interest included the afferent artery, site of anastomosis, draining veins as far as central veins, and arterial tree distal to the AVF to evaluate the steal phenomenon. All vessels were examined in both longitudinal and transverse planes, first in B mode followed by color Doppler evaluation. Arterial and venous diameters, patency, flow characteristics including peak systolic velocity (PSV) and end-diastolic velocity, PSV ratio (PSV in stenotic area/PSV upstream to the stenotic area), spectral waveforms, and presence or absence of thrombosis were documented. Any extraluminal seromas/hematomas or foci of infection were evaluated. Direct characteristics of the area of stenosis were luminal diameter reduction >50%, PSV >400 cm/s, PSV ratio >/=3, pronounced aliasing, high resistance Doppler waveform, reduction in access flow volume.[48]
Indications of Endovascular treatment for Non-Thrombosed Fistulas:[6] Clinical or hemodynamically significant dialysis circuit abnormalities and stenosis of >50% of the lumen on color Doppler examination in either venous outflow or arterial inflow.
Indications of Endovascular treatment for Thrombosed Fistulas:[6] Peri-anastomotic stenosis with thrombosis. Underlying venous stenosis as 85%–90% cases of venous stenosis are associated with thrombosis.
Indications of Treatment of Central Venous Stenosis:[6] Along with hemodynamically significant stenosis, clinical parameters such as arm swelling or frequently failing accesses. Angioplasty is the first-line treatment; however, associated primary stenting may be done with angioplasty, or stenting is done in case of >50% residual stenosis post angioplasty.
Endovascular procedure
Pre-procedure: Patient counseling was done in detail for the need for procedure, technique, complications, and expected outcomes. Pre-procedure investigations included duplex examination, renal function tests, and previous history for allergy to contrast or any other drugs. Informed consent was taken for the endovascular procedures after due discussion.
Devices & Personnel: MINDRAY DC-30 ultrasound machine was used for doing pre-procedure and intraprocedure sonographic evaluation. All percutaneous endovascular procedures were performed using the ALLENGERS Life HP interventional suite machine. All interventional procedures were done by the same team consisting of vascular interventional radiologists and their technical and nursing staff.
Fistulography and Angioplasty: After proper antiseptic precautions, the procedure was done under local anesthesia. Transradial or transvenous access was obtained and radial sheath (usually 6–7 F) was inserted in the arterial or venous limb of the fistula or femoral vein. A diagnostic fistulogram was done after flushing the sheath with 5000 IU heparin. A guidewire, preferably 150/260 cm, 0.035″ angled hydrophilic guidewire (Terumo), was then passed through the sheath up to the level of the central veins. 5F Kempe Access/MPA1 catheters were used over the wire and manipulated till they reach the site of the fistula. A balloon was introduced and passed over till the site of stenosis (6.00 mm for venous stenosis, 4–6 mm for juxta-anastomotic lesions, and 12–14 mm for central veins). It was inflated at high pressures multiple times for 3–5 min until the stenosis was dilated. Difficulties in stenosis dilatation were addressed using high-pressure balloons, shorter balloons, and longer duration of inflation. Fistulogram was done post procedure till the central veins to ensure patency and observe residual stenosis. The puncture site was closed by compression for 10 min.
Thromboaspiration: Access to the thrombosed segment was obtained via transarterial or transvenous puncture, and a 6–7-F access sheath was inserted. A preprocedural injection of sheath with 5000 U of heparin was done. A diagnostic angiogram was obtained to delineate the exact site of dysfunction. Thereafter, a hydrophilic-coated, steerable guidewire was advanced into the vessel over which an angiographic catheter was inserted with the tip of the catheter near the thrombosed segment. Catheter-directed thrombolysis was attempted through pulse spray technique injection of rt-PA via side hole catheters. Thereafter, thromboaspiration was performed using Penumbra's Indigo Aspiration System with CAT-6 catheters along with the simultaneous injection of heparin (3000–5000 U). After thromboaspiration, various sized balloons (4–6 mm) were used for angioplastic dilatation of the stenosed segment. A post-procedural angiogram was taken, and any residual thrombi were addressed with mechanical suction. The sheath was removed after completion of the procedure, and puncture site hemostasis was achieved by manual compression.
Stenting: Primary stenting along with PTA was done only in CVS in the study group. The stenotic central venous segment was completely effaced by an angioplasty balloon prior to stent deployment. Self-expanding, non-covered, and approximately 10% oversized stents were deployed post angioplasty. A post-procedural angiogram was taken.
Follow up: Medical management with low-molecular-weight heparin was done in successful cases for 5 days. On OPD follow-up, patients were observed for clinical improvement in limb swelling/palpable thrill, presence of any complications, and patency of AV fistula.
Statistical analysis
Continuous variables were assessed as mean. Categorical variables were studied as percentages. Tests of association were done by Chi-square test or Fisher's exact test wherever suitable. P < 0.05 was taken as significant. Kaplan–Meier survival analysis was done to analyze the short-term patency at 3 months follow-up. All statistical analysis was done using Graph Pad 9.7 and SPSS version 28.
Results
The study group comprised 46 patients who underwent endovascular treatment for dysfunctional hemodialysis fistulas at our department during the study period. The study group consisted of patients ranging from 29 to 80 years of age with a mean age of 50.90 years. Maximum patients presented in the sixth decade. Males dominated the study population (n = 29). Hypertension was the most prevalent comorbidity (n = 32, 72.72%) followed by diabetes (n = 25, 56.81%). The demographic profile of the study population is depicted in Figure 1 and Table 1.
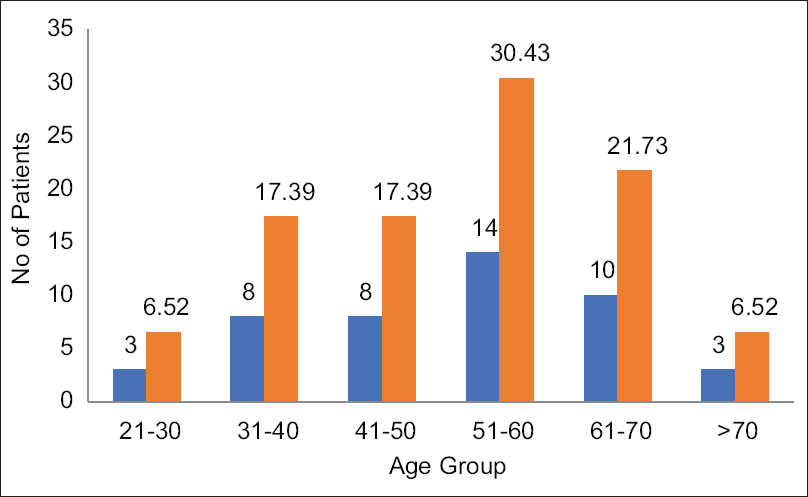
- Age distribution of the study group
| No. of patients | % | Technical Success | Clinical Success | P | |
|---|---|---|---|---|---|
| GENDER | |||||
| MALE | 29 | 63.04 | 27 | 24 | 0.3429 |
| FEMALE | 17 | 36.95 | 14 | 13 | |
| CO-MORBIDITIES | |||||
| Diabetes | 25 | 56.81 | 20 | 16 | 0.3244 |
| Hypertension | 32 | 72.72 | 28 | 23 | 0.5911 |
| Cardiac disease | 6 | 13.63 | 4 | 3 |
Out of 46 patients, 36 had stenosis at the fistula site and had to undergo PTA. Accessory veins were observed in three cases, and aneurysmal dilatation on the venous side of the fistula was seen in two cases. These patients were referred to a vascular surgeon for further management. Furthermore, 19 out of these 36 patients who had associated thrombosis underwent additional pharmacomechanical thromboaspiration. The rest of 10 patients, had CVS for which endovascular stenting was done after PTA.
It was observed that left-sided fistulas (n = 30, 65.21%) were more common than right-sided (n = 16.34.78%) fistulas. The most common anatomic site of fistulas in the study group were brachiocephalic (n = 24, 52.17%), followed by radio cephalic (n = 19, 39.13%) fistulas. The least common variety in the study group was brachio-basilic fistulas (n = 4, 8.69%). Among the central veins, the most common site of narrowing was subclavian vein (n = 6) followed by brachiocephalic and axillary veins in four cases each. Most of the patients presented to us after 1 year of fistula creation (n = 25, 54.34%), while 18 patients (39.13%) presented within 6 months of fistula formation. Fistula characters are depicted in Table 2.
| No. of patients (n=46) | % | Technical Success (n=41) | Clinical Success (n=37) | P (<0.05=Significant) | |
|---|---|---|---|---|---|
| Variables | |||||
| Radio-cephalic | 18 | 39.13 | 17 | 16 | 0.6343 |
| Brachio-cephalic | 24 | 52.17 | 21 | 19 | 1.00 |
| Brachio-basilic | 4 | 8.69 | 3 | 2 | 0.3794 |
| Age of fistula | |||||
| <6 months | 18 | 39.13 | 15 | 12 | 0.3655 |
| 6 months-1 year | 3 | 6.52 | 2 | 2 | |
| >1 year | 25 | 54.34 | 24 | 23 | 0.1628 |
The most common cause of dysfunction within the fistula was juxta-anastomotic stenosis seen in 33 of 36 patients of AVF stenosis, which comprised 91.66% of the subgroup. This was followed by venous and arterial stenosis/thrombosis in 11 and four cases, respectively. In most of the cases of CVS, the length of the dysfunctional segment was more than 5 cm, while a segment length of less than 3 cm was common in patients presenting with only juxta-anastomotic narrowing. The mean dysfunctional segment length in the study group was 5.08 cm. The profile of dysfunctional AVFs is depicted in Table 3.
| Variable | No. Of patients | % | Technical Success | Clinical Success |
|---|---|---|---|---|
| Type of Dysfunction | n=46 | n=41 | n=37 | |
| Stenosis | 46 | 100 | 41 | 37 |
| Thrombosis | 19 | 41.30 | 16 | 14 |
| Accessory veins | 4 | 8.69 | 3 | 0 |
| Aneurysmal dilatation | 2 | 4.34 | 1 | 1 |
| Site of stenosis | ||||
| Juxta-anastomotic | 33 | 71.73 | 28 | 26 |
| Venous | 11 | 23.91 | 7 | 5 |
| Arterial | 4 | 8.69 | 2 | 1 |
| Central veins | 10 | 21.73 | 10 | 10 |
| Cephalic arch | 2 | 4.34 | 0 | 0 |
| Length of Dysfunctional Segment | ||||
| Up to 3 cm | 13 | 28.26 | 12 | 11 |
| 3-5 cm | 18 | 39.13 | 16 | 14 |
| >5 cm | 15 | 32.60 | 13 | 12 |
Angioplasty balloon dilatation was done in 17 cases, out of which 15 resulted in technical success (88.23%). Out of these, 13 cases underwent at least one hemodialysis session and were marked as clinical successes (76.43%). Additional pharmacomechanical thromboaspiration was required in 19 cases, which resulted in a lower technical and clinical success rate of 84.2% and 73.6%, respectively. Endovascular balloon angioplasty and stenting was done for all 10 cases of CVS, which had a 100% success rate [Figure 2].

- Success rates of various endovascular procedures (PMT = Pharmacomechanical Thromboaspiration)
Technical failure was observed in five cases (10.86%). The reason for technical failure was cephalic arch stenosis in two cases, where stenosed segments could not be cannulated and accessory veins in one case. In all cases with technical failure, the stenotic segments had thrombosis in the juxta-anastomotic segment or adjacent arterial or venous channels.
Post-procedure complication rate was low, with one patient presenting with acute thrombosis and one patient with puncture site hematoma.
Overall technical successes after a single endovascular intervention were seen in 41 patients (89.13%). Patients had undergone hemodialysis on the next day of the endovascular procedure, and 37 patients could have at least one successful session of hemodialysis post procedure, yielding a clinical success rate of 80.43%. Within the first week of procedures, three cases presented with reocclusion, one of them with acute thrombosis. Re-intervention was attempted in all three patients, out of which two were successfully opened and underwent dialysis sessions. Patients were followed up at 1 and 3 months in case of optimal dialysis sessions or on an emergent basis as per requirement. Angioplasty with thromboaspiration was attempted in a patient with re-occlusion at 1 month; however, it had to be abandoned. Another reattempt at angioplasty was done for a restenosis of juxta-anastomotic segment occlusion and was successful. The PIPP for the overall study population was 82.60% at 1 week, 80.43% at 1 month, and 78.26% at 3 months. The PIAPP was 86.95% at 1 week, 84.78% at 1 month, and 82.60% at 3 months [Table 4 and Figure 3]. A representative case is shown in Figure 4.

- Kaplan–Meier graphs depicting the survival analysis for post-intervention primary patency and post-intervention assisted primary patency in the study group

- (a) Pre-procedure angiogram shows juxta-anastomotic stenosis in radio cephalic fistula with non-opacification of cephalic venous channels. (b): Balloon dilatation of the stenotic segment. (c) Post-procedure angiogram shows technical success with the near-complete opening of stenotic site and opacification of arterial, juxta-anastomotic, and venous channels
| Post-Intervention Primary Patency | Post-Intervention Assisted Primary Patency | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Time | Technical Success | % | Clinical Success | % | Technical | % | Clinical | % | |
| Total Study | 1 week | 38 | 82.60 | 34 | 73.91 | 40 | 86.95 | 36 | 78.26 |
| Population (n=46) | 1 month | 37 | 80.43 | 33 | 71.73 | 39 | 84.78 | 35 | 76.08 |
| 3 months | 36 | 78.26 | 32 | 69.56 | 38 | 82.60 | 35 | 76.08 | |
| Angioplasty (n=17) | 1 week | 13 | 76.4 | 11 | 64.7 | 15 | 88.23 | 13 | 76.47 |
| 1 month | 13 | 76.4 | 11 | 64.7 | 15 | 88.23 | 13 | 76.47 | |
| 3 months | 12 | 70.5 | 10 | 58.8 | 14 | 82.35 | 12 | 70.58 | |
| Angioplasty + Thromboaspiration (n=19) | 1 week | 15 | 78.9 | 13 | 68.42 | 15 | 78.94 | 13 | 68.42 |
| 1 month | 14 | 73.7 | 12 | 63.15 | 14 | 73.68 | 12 | 63.15 | |
| 3 months | 14 | 73.7 | 12 | 63.15 | 14 | 73.68 | 13 | 68.42 | |
It was observed that stenotic dysfunctional segments undergoing angioplasty dilatation had better technical (88.23%) and clinical success rates (76.47%) than thrombotic dysfunctional segments that underwent additional thromboaspiration with PTA (technical success rate: 84.2%; clinical success rate: 73.6%). However, at the end of 3-month follow-up, it was observed that the thrombotic dysfunctional segments had better PIPP (73.7%); in contrast, once re-intervention was done, the PIAPP was better in the stenotic subgroup undergoing angioplasty dilatation (82.37%).
Discussion
AVFs have been the cornerstone for hemodialysis in ESRD patients for the past many years. Among other options of grafts and tunneled catheters, AVFs have the advantages of being less prone to infections, better patency, and lower overall morbidity. Hemodynamically significant stenosis is a common occurrence in AVFs and may require multiple attempts of endovascular treatments in the form of PTA with or without thrombolysis. When the stenotic segments involve the central veins, PTA may be accompanied or followed by stenting to maintain patency.[910]
The demographic profile of the study group showed male predominance (n = 29, 63.04%), with the most common decade of presentation being the sixth decade.[91112] There was high prevalence of hypertension and diabetes in the study group, similar to the results of Al Gaby et al.[12] and Hendawy et al.[4] This is compatible with the fact that diabetic nephropathy is the most common cause of chronic renal disease in the Indian population.[1]
As per the anatomical site, the best post-procedural success was seen in radio cephalic fistulas (94.4%), followed by brachiocephalic fistulas (87.5%).[12] The most common site of stenosis was juxta-anastomotic segments (n = 33, 71.73%), followed by venous (n = 11, 23.91%) and arterial stenosis (n = 4, 8.69%). Most successful outcomes were seen in the juxta-anastomotic segmental stenosis with 84.84% success, followed by venous stenosis with 63.63% success. Involvement of cephalic arches in two cases led to failures of PTA due to non-cannulation of the stenosed segments. CVS was successfully opened in all 10 cases who underwent PTA and stent placement. The profile of dysfunctional segment in the study group was similar to the findings of Takahashi et al.[7] and Le et al.[13]
The overall technical success rate in the study group was 89.13%, and the clinical success rate was 80.43%. This may be attributed to the fact that most patients presented to us after 1 year of fistula formation, which has been related to better endovascular procedural results in the literature.[12] Similar observations were made by Heye et al.[10] with technical success rates of 87.1% and a clinical success rate of 73.2% after PTA in their study group. They also observed that radio cephalic fistulas had the highest PTA success rates of 94%. While studying stenotic fistulas, Aktas et al.[9] reported a technical success rate of 96.3% with a recurrence rate of 23.2% in short-term follow-up. Hendawy et al.[4] reported a success rate of 88.3% while studying dysfunctional fistulas. Machado et al.[14] reported a 91% success rate for endovascular procedures in stenotic arteriovenous fistulas.
In patients with associated thrombosis, success rates in the published literature range from 60% to 100%.[1516] For thromboaspiration, Çildağ et al.[11] reported a technical success rate of 83%, comparable to the results of present study (84.2%, n = 16).
CVS has been typically addressed with PTA, with high technical success rates of 70%–90%. However, recurrent stenosis post PTA yields considerably lower primary patency rates of 12%–50% at 1 year.[17] Stenting with metallic stents earlier and now with covered stents is often done along with PTA to improve long-term patency in CVS. Stenting may be done after failed PTA with recurring stenosis or primarily along with PTA.[17] The technique of PTA with primary stenting was followed in the present study group. Following the same, all ten patients of CVS were taken up for PTA and stenting with a 100% success rates and 100% primary patency at the end of 3 months. Ashwal et al.[18] also reported 100% success in ten patients of CVS undergoing PTA and stenting.
Because the durability of hemodialysis fistulas is limited and previous literature suggests primary patency rates of 26%–62% at the end of 1 year, it is essential to follow up patients after endovascular treatment to assess the patency rates after various procedures in setting of a multitude of anatomical and clinical variables.[9] After confirmation of clinical success as proved by at least one optimal hemodialysis sitting post intervention, patients were followed up at 1 and 3 months after the first intervention procedure. Wherever required, re-intervention was done by PTA with or without thromboaspiration.
The PIPP was 78.26% and PIAPP was 76.08% at the end of 3 months in the total study population. With better PIPP in the PTA plus thromboaspiration subgroup at 73.7% in comparison to the PTA subgroup (70.5%), it was deciphered that requirement of re-intervention was slightly more in the stenotic-only subgroup within the follow-up period. On the contrary, once re-intervened, PIAPP was higher in the PTA subgroup at 82.35% compared to those fistulas where stenosis was associated with thrombosis (73.68%), thereby indicating that re-thrombosis after primary intervention is related with early fistula failure. Recurrent endovascular injury in multiple procedures and associated comorbid factors that have been associated with reduced patency time periods can also be the reason of a lower PIAPP in this subgroup.[8]
Hendawy et al.[4] and Reffat H et al.,[19] while studying similar fistula profiles, reported a primary patency rate of 82% and 81%, respectively, at 3 months follow-up. Çildağ et al.[11] reported that post thromboaspiration, primary patency rates were as low as 55% at 3 months. In a multicenter prospective trial by Huijbregts HJ et al.,[20] PIPP and PIAPP at the end of 3 months were documented as 83% and 92%, respectively; however, their study population had a more homogenous profile of dysfunctional fistulas.
Overall, the results of PTA versus PTA with pharmacomechanical thromboaspiration were comparable in our study group. Although a slight edge was seen in the post-procedural patency after multiple procedures in the angioplasty group, the difference was not statistically significant.
The profile of AV fistulas associated with most successful outcomes post endovascular intervention was radio-cephalic fistulas that were formed more than 1 year ago, with juxta-anastomotic narrowing and a mean length of dysfunctional segment <3 cm. Cephalic arch stenosis and accessory veins had the worst post-intervention outcome in our study group.
Limitations
A modest study group size was the major limitation of the present study. Some aspects of patient profile could not be assessed, such as time to intervention from the onset of stenosis/thrombosis, previous detailed surgical history, and time to primary failure of previous AVFs. A short-term follow-up for patency assessment was also one of the limitations.
Conclusion
Endovascular intervention is the first-line treatment in dysfunctional arteriovenous fistulas as there is a multitude of options available for a variety of dysfunctions. Percutaneous angioplasty dilatation for stenotic dysfunction and angioplasty dilatation combined with thromboaspiration for thrombosed segments have comparable technical success rates and short-term patency. Angioplasty dilatation along with primary stenting for central venous stenosis has excellent technical success and notable short-term patency.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The incidence of end-stage renal disease in India: A population-based study. Kidney Int. 2006;70:2131-3.
- [Google Scholar]
- Arteriovenous fistulas and their characteristic sites of stenosis. Am J Roentgenol. 2015;205:726-34.
- [Google Scholar]
- A national study of autogenous arteriovenous access use and patency in a contemporary hemodialysis population. J Vasc Surg. 2019;69:1889-98.
- [Google Scholar]
- Endovascular treatment of failing arterio-venous fistula for hemodialysis. Syst Rev Pharm. 2021;12:259-64.
- [Google Scholar]
- ACR-SIR Practice Guideline for Endovascular Management of the Thrombosed or Dysfunctional Dialysis Access. Reston, VA: Digest of Council Actions; 2006. amended 2017
- [Google Scholar]
- Quality improvement guidelines for percutaneous image-guided management of the thrombosed or dysfunctional dialysis circuit. J Vasc Interv Radiol. 2016;27:1518-30.
- [Google Scholar]
- Endovascular arteriovenous dialysis fistula intervention: Outcomes and factors contributing to fistula failure. Kidney Med. 2020;2:326-31.
- [Google Scholar]
- Percutaneous endovascular treatment of stenosis of dialysis arteriovenous fistulas. Asian J Med Radiol Res. 2020;8:21-7.
- [Google Scholar]
- Percutaneous transluminal balloon angioplasty in stenosis of native hemodialysis arteriovenous fistulas: Technical success and analysis of factors affecting postprocedural fistula patency. Diagn Interv Radiol. 2015;21:160-6.
- [Google Scholar]
- Factors influencing technical success and outcome of percutaneous balloon angioplasty in de novo native hemodialysis arteriovenous fistulas. Eur J Radiol. 2012;81:2298-303.
- [Google Scholar]
- Percutaneous treatment of thrombosed hemodialysis arteriovenous fistulas: Use of thromboaspiration and balloon angioplasty. Clujul Med. 2017;90:66.
- [Google Scholar]
- Transradial approach for percutaneous intervention of malfunctioning arteriovenous accesses. J Vasc Surg. 2015;61:747-53.
- [Google Scholar]
- Results of endovascular procedures performed in dysfunctional arteriovenous accesses for haemodialysis. Port J Nephrol Hypert. 2012;26:266-71.
- [Google Scholar]
- Manual catheter-directed aspiration and other thrombectomy techniques for declotting native fistulas for hemodialysis. J Vasc Interv Radiol. 2001;12:1365-71.
- [Google Scholar]
- Salvage of thrombosed arteriovenous fistulae of patients on hemodialysis: Report on the experience of a Brazilian center. J Bras Nefrol. 2018;40:351-9.
- [Google Scholar]
- Endovascular interventions for central vein stenosis. Kidney Res Clin Pract. 2015;34:228-32.
- [Google Scholar]
- Percutaneous intervention for symptomatic central vein stenosis in patients with upper limb arteriovenous dialysis access. Indian Heart J. 2018;70:690-8.
- [Google Scholar]
- Assessment of the effectiveness of percutaneous transluminal balloon angioplasty for failing or nonmaturing arteriovenous fistulae for hemodialysis. Ann Vasc Surg. 2015;29:1363-7.
- [Google Scholar]
- Hemodialysis arteriovenous fistula patency revisited: Results of a prospective, multicenter initiative. Clin J Am Soc Nephrol. 2008;3:714-9.
- [Google Scholar]




