

Translate this page into:
An Unusual Case of High-Grade Non-Hodgkin Lymphoma Masquerading as Acute Pyelonephritis with Acute Kidney Injury
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Renal involvement in non-Hodgkin lymphoma (NHL) has myriad of morphological features. We discuss an unusual case who presented as acute pyelonephritis (leucocytosis and acute kidney injury), ovarian mass and compressive myelopathy finally diagnosed as Non Hodgkins Lymphoma.
Keywords
Acute pyelonephritis
leucocytosis
non hodgkin lymphoma

Introduction
Renal involvement in non-Hodgkin lymphoma (NHL) has been reported to present with glomerulonephritis, acute kidney injury (AKI), and lymphoma infiltrating the kidney parenchyma.[1] We discuss an unusual case who presented with acute pyelonephritis (leucocytosis and acute kidney injury), ovarian mass, and compressive myelopathy and was finally diagnosed as NHL.
Case Report
A 43-year-old married female was admitted to our hospital with history of fever, right side flank pain, and burning micturition. Fever subsided in a week after symptomatic medication. Pain was both in flank and lower back region, used to get relieved with medication, non-radiating, not associated with aggravating factors. There was no history of weight loss, night sweats, anorexia. She had been recently diagnosed with type 2 diabetes mellitus and hypertension and was on insulin during hospital stay and amlodipine; but fundus examination was not suggestive of diabetic retinopathy. General examination; pulse rate- 88/min, BP- 130/90 mmHg. On systemic examination she had right side renal angle tenderness.
Laboratory examination showed; TLC of 57,000 with polymorphs of 80%, urine routine suggestive of protein of 1+, RBC 3-5 and pus cells 5-8 per high power field, blood urea 60 mg/dl, creatinine 3.2 mg/dl, 24 h urinary protein 1,600 mg/day. Ultrasonography was suggestive of normal sized kidneys, with left adnexal hypoechoic cyst of size 5.4 × 4.8 cm with internal echoes suggestive of hemorrhagic ovarian cyst. Her urine and blood cultures were sterile and procalcitonin level was less than 0.5 ng/ml. Initially she was diagnosed as acute pyelonephritis (APN) and managed with intravenous antibiotics. In view of persistent leucocytosis even after treatment with antibiotics, to rule out leukemoid reaction and to look for the infiltration of lymphoma, bone marrow aspiration and biopsy was done, which was suggestive of reactive marrow with myeloid hyperplasia., Few marrow spaces showed focal areas of likely early fibrosis (grade 1 on Reticulin stain).
Serum tumor markers were within normal limits with slightly elevated CA125. Ultrasound with doppler didn't show any evidence of ovarian torsion. Contrast enhanced CT chest and abdomen revealed heterogeneously enhancing solid mass measuring 6.5 × 4.8 × 4.8 cm in pelvis likely arising from left ovary [Figure 1a]. In view of acute persistent pain, she underwent right side salpingoophorectomy [Figure 1b]. After the operation her pain abdomen reduced.
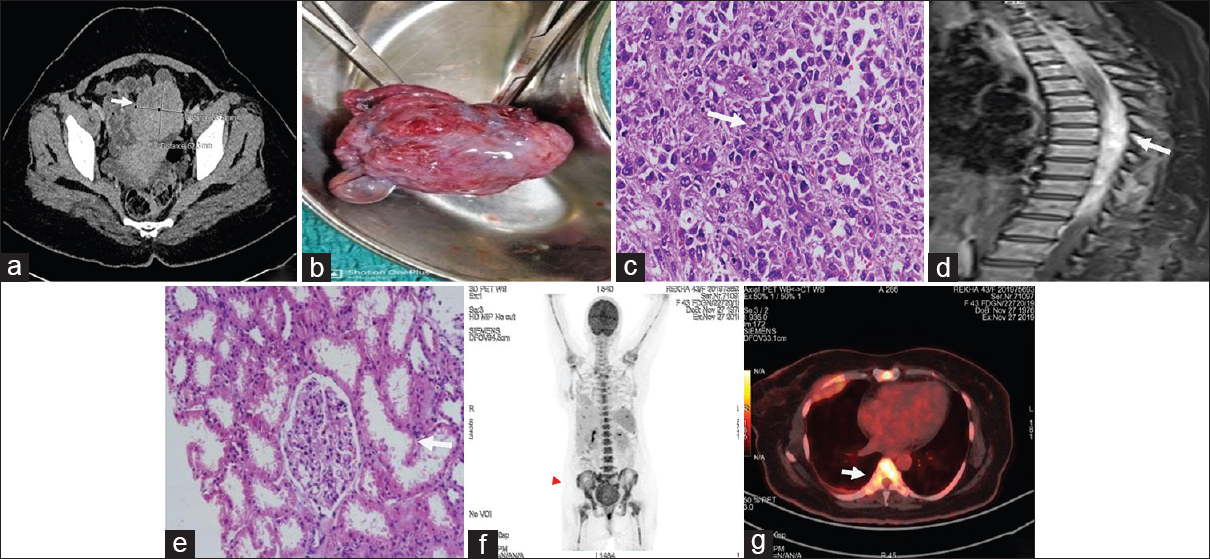
- (a) CECT abdomen suggestive of heterogeneously enhancing solid mass measuring 6.5 × 4.8 × 4.8 cm in pelvis arising from left ovary. (b) gross specimen of left ovary measuring 6 × 5 × 3 cm showing enlarged ovary with attached fallopian tube. (c) ovarian mass histology showing atypical cells which are highly pleomorphic and show hyperchromatic nucleus with coarse chromatin. (d) long segment infiltrating lesion in right epidural space extending from D4 to D10 vertebral level. (e) renal histology showing normal glomerulus. (f and g) PET CT showing increased uptake in bone marrow
Histopathology of the ovarian mass showed fibrocollagenous tissue infiltrated by singly lined atypical cells predominantly arranged in sheets and focally in loose nests and alveolar pattern [Figure 1c]. The tumor cells were highly pleomorphic and showed hyperchromatic nucleus with coarse chromatin. Brisk mitotic activity was seen. Native ovarian parenchyma was not identified in the multiple sections examined. Sections from the fallopian tube showed infiltration of the mucosa by similar tumor cells. Large panel of immunohistochemistry markers including PLAP, AFP, EMA, Cytokeratin, ER, PR, Inhibin, S100, SMA, Desmin, Vimentin, CD99, and synaptophysin were negative. It was followed by lymphoma panel including CD20, CD79a, CD45RO, CD3, CD34, CD 30, CD43, and Cd68. Tumor cells were positive for LCA and CD43 while CD 68 showed focal positivity. Rest of the markers were negative. A diagnosis of hematolymphoid malignancy was made. Another IHC panel applied for further characterization of malignant cells included CD117, Tdt, MPO, CD56, CD4, and CD8 turned out to be negative. High grade NHL, unclassified probably monocytic leukemic infiltration was the final diagnosis.
During hospital stay she developed bilateral lower limb weakness and urinary retention and on examination had sensory level at D10 vertebra. As per the neurologist's opinion she underwent MRI dorso-lumbar spine which was suggestive of long segment infiltrating lesion in right epidural space extending from D4 to D10 vertebral level [Figure 1d].
In view of proteinuria and renal dysfunction she underwent renal biopsy which had 15 glomeruli that were largely unremarkable [Figure 1e]. Tubules showed acute tubular injury. Tubular atrophy and interstitial fibrosis involved about 20–30% of sampled cortex. Focal moderate to dense interstitial inflammation was noted comprising lymphocytes with few neutrophils. Direct immunoflourescence studies for IgG, IgA, IgM, C3, C1q, kappa and lambda were negative. Therefore, the renal biopsy impression kept was acute tubulointerstitial nephritis. 18FDG-PET/CT demonstrated bone marrow involvement characterized by a high 18FDG uptake [Figure 1f, g]. She has been offered treatment with CHOP plus rituximab regimen.but the family opted for alternative therapy.
Discussion
Pyelonephritis typically manifests with signs and symptoms of both systemic inflammation (e.g., fever, chills, and malaise) and bladder inflammation (e.g., urinary frequency, urgency, and dysuria). Bacterial pyelonephritis may be associated with acute kidney injury, particularly when the clinical presentation includes hypotension, obstruction to the flow of urine, and the use of nephrotoxic drugs or contrast agent. When it occurs in patients without obvious predisposing causes, the possibility of bacterial pyelonephritis is often not considered, and such cases may present diagnostic dilemmas. Similarly our case made us to look for other cause.[2]
Kidney involvement is an under-recognized complication of NHL. The diversity of lymphoma-related renal manifestations makes diagnosis difficult. While abrupt worsening of kidney function may be thefirst sign of malignant disease. Kidney manifestations encompass a broad spectrum of disease: prerenal acute kidney injury (AKI), acute tubular necrosis (ATN), renovascular disease, parenchymal infiltration, obstruction, glomerulopathies, and electrolyte and acid-base abnormalities.[1]
Glomerulopathies in NHL occur earlier and progress with disease. Proliferative lesions may account for up to 30% of glomerular diseases. However, in our case it is tubulointerstitial nephritis and acute tubular injury. It has been hypothesized that cytokines produced by lymphoma cells may cause tubular injury and interstitial fibrosis. Another explanation for kidney dysfunction is an elevated pressure in renal parenchyma caused by lymphocytic infiltration leading to compression of tubules and modifications in microvascular structure. Malignant lymphoid cells may occur in the ovary either as a primary neoplasm or as a secondary manifestation of a disseminated occult or known disease.[3] Only 1% of patients further diagnosed with malignant lymphoma present initially with ovarian enlargement.[4] Primary ovarian lymphoma, account for 0.5% of all NHL and 1.5% of all ovarian neoplasms.
CD45, CD20, CD79a are selective marker that recognizes a subpopulation of B-cells, CD3, CD 45RO, CD43 is the marker for T-cells and NK-cells, CD30 is the marker for activated T-cells and B-cells. Human leukocyte common antigen (LCA) is identified on B and t lymphocytes. CD45 immunoreactivity is recognized to be highly specific for NHLs. Markers of myeloid cells and monocytes are anti-myeloperoxidase, CD34, CD68, CD43.[5]
Lymphomas of the ovary can occur at any age, but most often in women over the age of 40.[6] The most common presenting signs or symptoms of malignant lymphomas involving the ovaries are abdominal or pelvic pain or mass. Fever, night sweats, fatigue, or weight loss (B symptoms) was noted in 10–33% of the patients. B- and T-cell NHL can arise in the ovary, but B-cell tumors are much more frequent. Both B- and T-cell NHL can arise in the ovary, but B-cell tumors are much more frequent. The histological differential diagnosis includes granulosa cell tumor, dysgerminoma, small-cell carcinoma of hypercalcemic type, granulocytic sarcoma, and poorly differentiated surface-epithelial or metastatic carcinoma.[7]
Our patient had leukocytosis for which no relevant explanation is found in literature. However, it is seen that leukocytosis or leukemoid reaction may develop in association with carcinomas of the lung and stomach.[8] Previous reports in literature similar to our case are mentioned in Table 1.
| Sl No | Title | Interesting features | Points mimic to current case | Year of publication | Reference |
|---|---|---|---|---|---|
| 1. | Renal lesions associated with malignant lymphomas | The incidence of lymphomatous infiltration of the kidneys in the whole series is 33.5 per cent | Our case has tubuleinterstitial nephritis | 1962 | American journal of medicine[9] |
| 2 | Non-Hodgkin’s lymphoma presenting with spinal cord compression; a clinicopathological review of 25 cases | Spinal cord compression (SCC) is an uncommon primary manifestation of NHL, occurring in less than 5% of newly diagnosed cases | Cases presented with spinal cord or cauda equina compression as the first symptom | 2000 | European Journal of Cancer[10] |
| 3. | Undifferentiated ovarian carcinoma associated with leukemoid reaction | presented with fever and abdominal pain WBC counts were up to 143,000/microl | WBC count in our patient was 50,000. | 2001 | Chinese medical journal.[11] |
| 4. | Kidney involvement and renal manifestations in non-Hodgkin’s lymphoma and lymphocytic leukemia: a retrospective study in 700 patients | The most common glomerular lesion reported is membranoproliferative GN, followed by membranous GN | Tubulointerstitial nephritis seen in our patient | 2002 | European Journal of haematology[12] |
| 5. | Renal impairment in patients with ovarian cancer | Reduction in renal function and dialatation of upper urinary tract is frequent in patients with ovarian cancer at the time of diagnosis | No dilatation of upper urinary tract seen in our patient | 2003 | European journal of obstetrics and gynaecology and reproductive biology[13] |
| 6. | Spinal cord compression secondary to metastatic non Hodgkins lymphoma: a case report. | Non-hodgkin’s lymphoma metastases to the spinal cord are not common, with an occurrence rate of 0.1% to6.5% | Metastasis to the thoracic spine is most common, followed, by metastasis to the lumbar spine | 2005 | Archives of Physical Medicine and Rehabilitation[14] |
| 7. | Renal Involvement in Non-Hodgkin Lymphoma: Proven by Renal Biopsy | CLL/SLL were the most common types of NHL associated with renal injury, and the most common pattern of glomerular lesion was MPGN-like pattern. | 40% patients showed lymphomatous infiltration of the interstitium. | 2014 | Public Library of Science (PLOS) ONE[15] |
| 8. | Clinical presentation and pathology spectrum of kidney damage in non-Hodgkin lymphoma/leukemia and lymphoplasmacytic lymphomas. | Clinical presentation of renal involvement in patients with NHL/CLL and LPCL include AKI, NS, proteinuria and/or hematuria, arterial hypertension or chronic kidney disease (CKD) | Interstitial nephritis was seen in 41.6% patients | 2015 | Journal of Leukemia |
Conclusion
This is an unusual case of NHL without bone marrow involvement presenting as ovarian mass, persistent leukocytosis, renal dysfunction mimicking acute pyelonephritis and paraparesis symptomatically improved after treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Kidney involvement in leukemia and lymphoma. Advances in chronic kidney disease. Elsevier 2014
- [Google Scholar]
- Non-Hodgkin's lymphoma presenting asadvanced ovarian cancer—a case report and review of literature. Int J Gynecol Cancer. 2005;15:554-7.
- [Google Scholar]
- Manual of diagnostic antibodies for immunohistology. London: Greenwich Medical Media; 1999. Manual of diagnostic antibodies for immunohistology London: Greenwich Medical Media;
- Primary non-Hodgkin's lymphoma of the ovary–a case report. J Clin Diagn Res. 2016;10:ED10-1.
- [Google Scholar]
- The spectrum of kidney involvement in lymphoma: A case report and review of the literature. Am J Kidney Dis. 2010;56:1191-6.
- [Google Scholar]
- Undifferentiated ovarian carcinoma associated with leukemoid reaction. Zhonghua Yi Xue Za Zhi (Taipei). 2001;64:592-6.
- [Google Scholar]
- Non-Hodgkin's lymphoma presenting with spinal cord compression; A clinicopathological review of 25 cases. Eur J Cancer. 2000;36:207-13.
- [Google Scholar]
- Kidney involvement and renal manifestations in non-Hodgkin's lymphoma and lymphocytic leukemia: A retrospective study in 700 patients. Eur J Haematol. 2001;67:158-64.
- [Google Scholar]
- Renal impairment in patients with ovarian cancer. Eur J Obstet Gynecol Reprod Biol. 2003;106:198-202.
- [Google Scholar]
- Spinal cord compression secondary to metastatic non-Hodgkin's lymphoma: A case report. Arch Phys Med Rehabil. 2005;86:332-4.
- [Google Scholar]
- Renal involvement in non-Hodgkin lymphoma: Proven by renal biopsy. PLoS One 20149:9.
- [Google Scholar]
- Clinical presentation and pathology spectrum of kidney damage in non-Hodgkin lymphoma/leukemia and lymphoplasmacytic lymphomas. J Leuk. 2015;3:2.
- [Google Scholar]




